Nair Shobita*, V Panneer Selvam, Shah Vinit J, Jayaraman Radha, V Vijayraghavan and Gupta Amal
Department of Cornea, Arasan Eye Hospital, Erode, Tamil Nadu, India
*Corresponding Author:Nair Shobita, Department of Cornea, Arasan Eye Hospital, Erode, Tamil Nadu, India.
Received: February 17, 2021; Published: March 06, 2021;
Aims and Objectives: To determine the correlation between central corneal thickness (CCT), Refractive errors, and corneal curvature. To investigate any association between Central corneal thickness (CCT) and variables, namely, age, refractive errors, mainly Myopia and Hypermetropia, Corneal curvature, and axial length.
Methods and Material: Observational Hospital-based Cross-sectional study of the data collected from patients with refractive errors presenting to the outpatient department (OPD) at our hospital. 240 eyes of 120 patients who met the inclusion criteria included in the study. Following examinations were performed for all the patients, measuring best-corrected visual acuity, central corneal thickness, corneal curvature by Topography, and axial length by A-scan ultrasonography. All patients underwent a complete slit-lamp examination.
Statistical Analysis:Correlation between central corneal thickness (CCT) and four factors, namely, age of the patient, degree of myopia and hypermetropia, corneal curvature, and axial length, was studied using Karl Pearson's correlation coefficient(r). We did data analysis with the SPSS 20.0 software.
Results:The mean central corneal thickness of our study population was 531.9 microns. The mean age of the overall study population was 27.02 years. The mean corneal curvature 44.34 D, and the mean axial length was 24.24mm. Central corneal thickness was significantly associated with corneal curvature.
Conclusions: Central corneal thickness has a negative correlation with Corneal curvature, i.e., as the corneal curvature increases, the central corneal thickness decreases, and vice versa. However, there was no significant association between Central corneal thickness and other parameters like Age, Degree of Myopia, Hypermetropia, and Axial length.
Keywords: Central Corneal Thickness;Myopia; Hypermetropia; Axial Length; Corneal Curvature; Correlation Analysis; Age
Central corneal thickness (CCT) is an essential parameter that helps assess the corneal barrier status, endothelial function, and in general, corneal well-being. Measuring CCT has emerged as a vital investigation in the diagnosis and management of corneal disorders. Furthermore, CCT is a measure of corneal rigidity and the amount of corneal tissue available for refractive surgery. The corneal thickness has a direct impact on intraocular pressure measurement and management of glaucoma. In recent years, various refractive procedures have developed, and corneal thickness is the most important deciding factor for the type of refractive surgery[1].
Four components determine the overall refractive state of the eye: Corneal power (mean- 43D), Anterior chamber depth (mean- 3.4mm), Crystalline lens power (mean- 21D), Axial length (mean- 24mm) [2].
There is still no clear consensus about the anterior segment's changes occurring in hyperopic and myopic eyes. The axial length is well known to be shorter in hyperopes and longer in myopes than in emmetropic eyes. Applying the simple stretching theory similar to a balloon's inflation, we would expect the cornea to be thinner than average in myopes and thicker than average in hyperopes[3].
Several studies have assessed associations between the CCT and various factors such as age, gender, race, refractive error, and corneal curvature. In many studies, the results are unconvincing and, at times, contradictory. Some studies have reported no correlation between corneal thickness and myopia level, whereas some studies have found the cornea to be thinner in more myopic eyes[4-8]. Most of the studies have focused mainly on myopic eyes, but we have also included hyperopic eyes in our study.
Thus the present study is designed to determine the correlation between Refractive errors (Myopia and Hyperopia), corneal curvature, axial length with the central corneal thickness (CCT) in the South Indian population.
Observational Analytical Cross-sectional study of the data collected from patients with refractive errors presenting to the Outpatient department at our hospital. 240 eyes of 120 patients who met the inclusion criteria of age between 20-45 years, both the gender and refractive errors of myopia and hyperopia, were included in the study. The study was conducted after getting clearance from the hospital ethical committee and the scientific committee. All the patients gave written informed consent before enrolment in the study.
Patients with simple astigmatism, any corneal pathology like corneal edema, opacities, dystrophies, keratoconus, any lenticular pathology like cataract, lenticonus, any history of contact lens use within one month, an external eye disease like pterygium, history of trauma, retinal pathology Like Retinal detachment, retinitis pigmentosa were excluded. Systemic conditions like Marfans disease, Ehler-danlos, connective tissue disorders, any history of previous ocular surgery, and glaucoma were excluded from the study.
Visual acuity (BCVA) using Snellen's chart was measured, followed by retinoscopic refraction (Welch Allyn Streak retinoscope). Then central corneal thickness was measured using ultrasound pachymeter (PacScan300P Sonomed), corneal curvature by Topography (Oculus keratograph 5M), and axial length by A-scan ultrasonography (PacScan300A Sonomed). Detailed anterior segment evaluation using slit-lamp biomicroscopy and fundus findings were confirmed by slit-lamp biomicroscopy with a 90 D lens.
The refractive error was divided into four categories Low myopia (0 to -3D), Moderate (-3D to -6D), high myopia (>-6D), and hypermetropia (> +0D).
Data entry is done in Excel. We did data analysis with the help of SPSS 20.0 statistical software. Correlation between central corneal thickness (CCT) and four factors, namely, age of the patient, degree of myopia and hypermetropia, corneal curvature, and axial length, was studied using Karl Pearson's correlation coefficient(r) and represented on a Scatter plot diagram.
The mean age in the study was 27.02 years (Range 20-45 years).In the study, 45.0% (54 out of 120) of the patients are male, and 55.0 % (66 out of 120) are female. The male to female ratio was 0.81:1. The demographic data of the age, gender, refractive errors, and central corneal thickness in the study group are shown in table 1.
| Demographics | Frequency | Percentage |
|---|---|---|
Age |
||
20 - 25 Years |
150 |
62.5% |
26 - 30 Years |
38 |
15.8% |
31 - 35 Years |
10 |
4.2% |
36 - 40 Years |
8 |
3.3% |
41 - 45 Years |
34 |
14.2% |
Sex |
||
Male |
108 |
45.0% |
Female |
132 |
55.0% |
Central Corneal Thickness |
||
< 500 |
36 |
15.0% |
500 - 550 |
112 |
46.7% |
550 - 600 |
76 |
31.7% |
> 600 |
16 |
6.7% |
Refractive Errors |
||
Low Myopia |
108 |
45.0% |
Moderate Myopia |
84 |
35.0% |
High Myopia |
14 |
5.8% |
Hyperopia |
34 |
14.2% |
Total |
240 |
100.0% |
Table 1:Demographic data of the study population.
In the low myopia group (0 to -3D), the mean age is 24.29, SD 5.285, and the range is 20-43years. In the moderate myopia group (-3 to -6D), the mean age is 24.64, SD 4.951, and the range is 20-39years. In high myopia group (> -6D), mean age is 25.86, SD 7.862 and range is 20-43years. In hyperopia group (> +0D), mean age is 42, SD 7.053 and range is 40-45years(Table 2).
| Degree of Refractive Errors | Mean | SD | Range |
|---|---|---|---|
Statistics of Age in Years by Degree of Refractive errors |
|||
Low Myopia |
24.29 |
5.285 |
20 - 43 |
Moderate Myopia |
24.64 |
4.951 |
20 - 39 |
High Myopia |
25.86 |
7.862 |
20 - 43 |
Hyperopia |
42.00 |
7.053 |
20 - 45 |
Total |
27.02 |
8.254 |
20 - 45 |
Statistics of Central Corneal Thickness by Degree of Refractive errors |
|||
Low Myopia |
535.3 |
34.87 |
436 - 600 |
Moderate Myopia |
534.2 |
40.99 |
436 - 616 |
High Myopia |
512.2 |
26.79 |
469 - 567 |
Hyperopia |
523.3 |
32.58 |
469 - 599 |
Total |
531.9 |
36.80 |
436 - 616 |
Statistics of Corneal Curvature by Degree of Refractive errors |
|||
Low Myopia |
44.22 |
1.801 |
40.85 - 50.20 |
Moderate Myopia |
44.41 |
1.547 |
40.30 - 48.00 |
High Myopia |
44.46 |
1.533 |
42.90 - 48.05 |
Hyperopia |
44.50 |
1.433 |
42.20 - 47.75 |
Total |
44.34 |
1.645 |
40.30 - 50.20 |
Statistics of Axial Length by Degree of Refractive errors |
|||
Low Myopia |
24.01 |
0.865 |
21.68 - 25.94 |
Moderate Myopia |
24.89 |
0.898 |
23.10 - 26.91 |
High Myopia |
26.62 |
1.681 |
24.03 - 29.77 |
Hyperopia |
22.42 |
0.913 |
20.34 - 23.79 |
Total |
24.24 |
1.363 |
20.34 - 29.77 |
Table 2:Statistical data of refractive errors with age, central corneal thickness, corneal curvature, and axial length in our study cohort.
Table 2: Statistical data of refractive errors with age, central corneal thickness, corneal curvature, and axial length in our study cohort.
In the low myopia group (0 to -3D), the mean central corneal thickness is 535.3microns, SD 34.87microns, and range is 436-600 microns. In the moderate myopia group (-3 to -6D), the mean central corneal thickness is 534.2, SD 40.99, and range is 436-616 microns. In the high myopia group (> -6D), the mean central corneal thickness is 512.2, SD 26.79, and the range is 469-567microns. In hyperopia group (> +0D), mean central corneal thickness is 523.3, SD 32.58 and range is 469-599microns (Table 2).
The mean corneal curvature (K) in the low myopia group is 44.22 D, SD 1.801, and range 40.85 - 50.20D. Mean corneal curvature (K) in the moderate myopia group is 44.41 D, SD 1.547 and range 40.30 – 48.00 D and in the high myopia group is 44.46 D, SD 1.533 and range 42.90 – 48.05 D. Mean corneal curvature (K) in the hyperopia group is 44.50D, SD 1.433 and range 42.20 – 47.75 D(Table 2).
The mean axial length in the low myopia group is 24.01 mm, SD 0.865, and range 21.68 - 25.94 mm. The mean axial length in the moderate myopia group is 24.89, SD 0.898, and range 23.10 - 26.91 mm, and in the high myopia group is 26.62 mm, SD 1.681, and range 24.03 - 29.77 mm. The mean axial length in the hyperopia group is 22.42 mm, SD 0.913, and range 20.34 - 23.79 mm (Table 2).
The correlation between central corneal thickness and various parameters like age, myopia, hyperopia, central corneal thickness, and axial length in our study are shown in table 3. The p-value is greater than the significance level 0.05; thus, there was no correlation between central corneal thickness and age, myopia, hyperopia, and axial length. A straight line in the scatter plot parallel to the x-axis confirms no correlation between central corneal thickness and age, myopia, hyperopia, and axial length (Figure1-4).
| Karl Pearsons correlation analysis | Correlation coefficient (r) | P-value |
|---|---|---|
CCT and Age |
-0.121 |
0.062 |
CCT and Myopia |
0.129 |
0.065 |
CCT and Hyperopia |
-0.161 |
0.362 |
CCT and Corneal Curvature |
-0.326 |
0.001 |
CCT and Axial Length |
0.085 |
0.191 |
Table 3:Correlation between CCT and various parameters in the study.
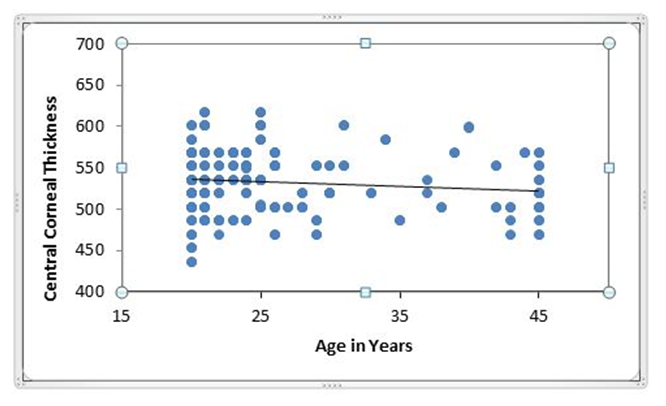
Figure 1:Correlation between Central Corneal Thickness and Age.
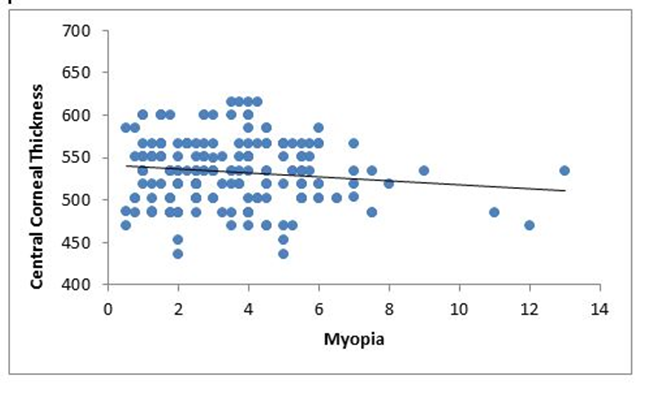
Figure 2:Correlation between Central Corneal Thickness and Myopia.
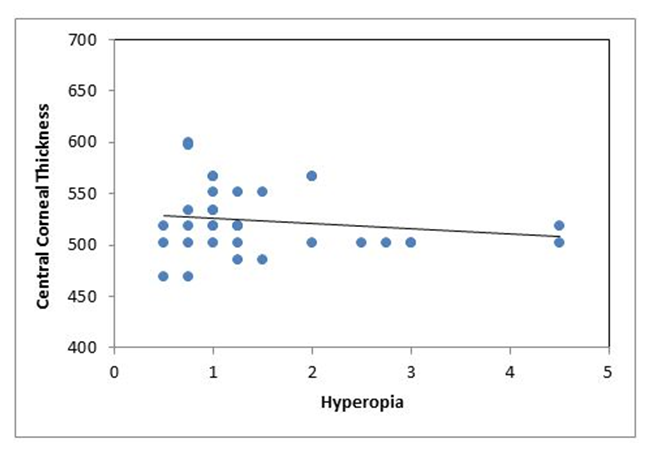
Figure 3:Correlation between Central Corneal Thickness and Hyperopia.
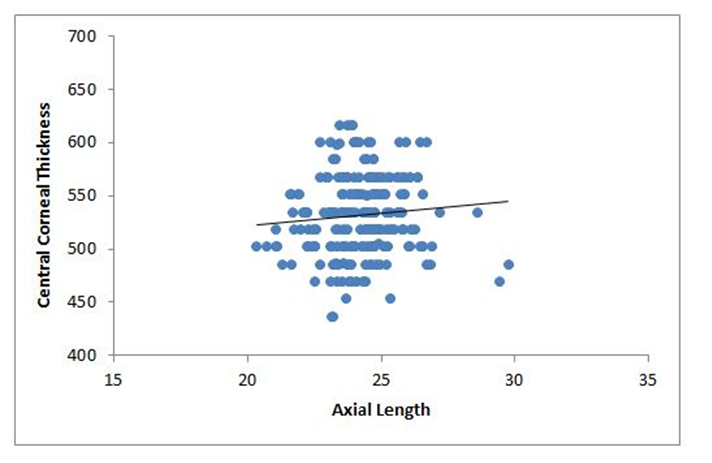
Figure 4:Correlation between Central Corneal Thickness and Axial Length.
A statistically significant correlation between central corneal thickness and corneal curvature was noted in our study (Table3). The p-value is less than the significance level 0.05; thus, there is a correlation between central corneal thickness and corneal curvature. The negative sign implies that the correlation is negative. Central corneal thickness will increase with a decrease in corneal curvature, and central corneal thickness will decrease with an increase in corneal curvature. A downward slope in the scatter plot (Figure 5).
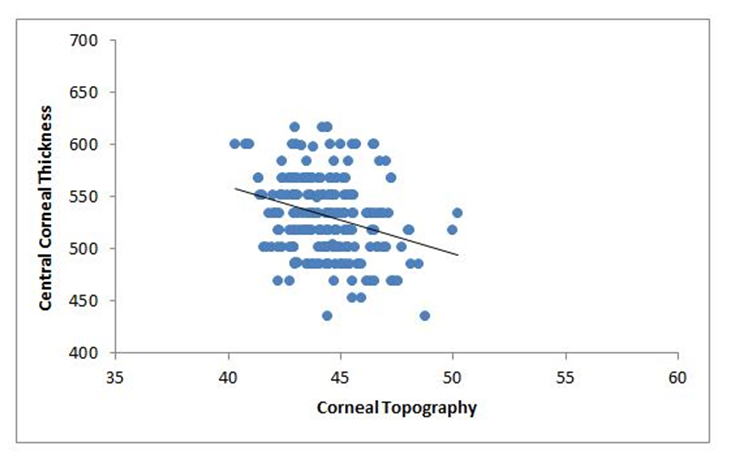
Figure 5:Correlation between Central Corneal Thickness and Corneal Curvature.
Our present study has attempted to determine the correlation between central corneal thickness and four variables, namely age, degree of myopia and hypermetropia, corneal curvature, and patient's axial length.
In our study, the mean age was 27.02 years, with a range of 20 to 45 years.S. Lee., et al.[9] in Korean myopes, reported patients' mean age as 30.05 years with a range from 22 to 46 years of age. B. Koucheki., et al.[10]said the study subjects' mean age was 28.7 ± 7.7 years, ranging from 18 to 55 years; these results matched our results. In our study, the male to female ratio is 0.81:1, which means most young refractive error patients are females. A. Elias., et al.[3] reported 62% of female patients, andS. Ortiz., et al.[11] in her study reported that 61.1% of female patients were similar to our research suggesting female preponderance in refractive errors. Muthukrishnan., et al.[12]reported identical mean age and female prevalence for refractive errors in their South Indian population study.
The mean central corneal thickness in our study is 531.9 microns and SD 36.80 microns. Muthukrishanan., et al.[12] reported a mean CCT of 533.87 +40.02, and L. Vijaya., et al.[13]reported the mean CCT (SD) in the south Indian population to be 511.4 (+33.50) microns. Nangia., et al.[14] in their study of the Central Indian population, reported thinner corneas with mean CCT of 514+ 33 microns.H. Fam., et al.[15] studies on 714 Chinese patients, had a mean central corneal thickness of 534.5 microns. S. Chang., et al.[16] in their study had 533 Doughty and Zaman[17], in his meta-analysis, reported the average CCT as 535 microns. These results were similar to our study. Contrary to our results, S. Ortiz., et al.[11]in herstudy, had the mean CCT of 544 ± 37 microns. M. Garcia., et al.[18] reported mean CCTof 550 ± 36microns, T. Almahmoud., et al.[19] also obtained a higher CCT value of 543 ± 34microns. These results are slightly higher than our study and may be due to genetic and racial variation in the study population.
In our study, the mean corneal curvature (K) in the overall study population was 43.34D. The mean corneal curvature (K) in the low myopia group is 44.22 D. The moderate myopia group is 44.41 D, in the high myopia group is 44.46 D. In the hyperopia group is 44.50D. B. Koucheki., et al.[10] found the average mean K in 340 study people was 43.9 ± 1.5 (Range, 40.1 to 47.6D). A. Elias., et al.[3] reported the mean corneal curvature was 43.68 diopters (SD 1.41, range 39.37D – 47.50D, median 43.62D). These results are similar to our study.
In our study, the mean axial length in the overall study population is 24.24mm. The mean axial length in the low myopia group is 24.01 mm, in the moderate myopia group is 24.89, in the high myopia group is 26.62 mm, in the Hyperopia group is 22.42 mm. S. Ortiz., et al.[11] reported mean axial length in myopia <6D group as 25.18 ± 1.16 mm, in myopia between 6 to 12D as 26.59 ± 1.26 mm and in myopia >12D group as 29.45 ± 2.58 mm. S. Chang., et al.[16] in their study reported mean axial length as 25.2mm in a study population of216 patients. Our results were comparable to studies conducted in different countries and races.
There was no statistically significant association between Central corneal thickness (CCT) and age (Pearson r = -0.121, P = 0.062).Our result is similar to a study done by Price., et al. [20] A. Elias., et al.[3] and S. Lee., et al. [9]found no correlation between CCT and age. In the studies by L.Vijaya., et al[13], E. Lee., et al.[21] showed an inverse relationship between age and CCT (Pearson r = -0.12; P < 0.0001), CCT decreased by 4.8micronsand 2.8 microns per decade, respectively. Lenskul., et al. [22]Foster., et al.[23] and Cho and Lam., et al. [24] found that central corneal thickness decreased with increasing age.
Von Bahr[25]first generated interest in the correlation between myopia and CCT in 1956, when he reported thinner corneas in myopia less than –4D.
Our study showed no statistically significant difference or correlation between Central corneal thicknesses and myopic refractive error (Pearson r = 0.129, P=0.065). This result is in agreement with the majority of previous studies. Liu Z[26], Pauline Cho., et al. [27]and Pedersen., et al. [28];found no significant association between the CCT and the amount of refractive error, which is similar to our study.Nemesure., et al.[29] reported thinner corneas in high myopic subjects, and Muthukrishnan., et al. [12] reported thicker corneas in high myopia, contrary to our study. In our study, there was no correlation between central corneal thickness and hypermetropia (r = -0.161, P = 0.362).B. Koucheki., et al.[10]Nemesure., et al.[29] and Pauline Cho., et al. [27]reported no correlation between positive spherical equivalent refractive error and the CCT similar to our study.
In the present study, there is negative correlation between central corneal thickness and corneal curvature (r = - 0.326, P = 0.001). A. Elias., et al.[3] found a negative correlation (Pearson r= -0.23)(P=0.001) between CCT and corneal curvature. Nangia., et al. [14] also reported a significant association of CCT with lower corneal power. The correlation was significant at the 0.001 level, which is similar to our study.A. Tomidokoro., et al.[30]reported a positive correlation of CCTwith corneal curvature in his study. This result did not match our study. Francis., et al.[31]Cho and Lam[24],reported no significant association between CCT and corneal curvature. These results did not match our study.
In our study, there is no correlation between central corneal thickness and axial length (AL) (r = -0.085, P = 0.191).J. Gros-Otero., et al.[32] reported no correlation between CCT and axial length. Muthukrishnan., et al.[12] reported a strong positive correlation between CCT and axial length. Nangia., et al. [14]showed a strong association of CCT with shorter axial length.S. Lee., et al.[9] reported a positive correlation between CCT and axial length in myopic Korean patients. CCT and AL had a positive correlation in the intermediate, high, and extreme myopic groups but not in the low myopic group.S. Chang., et al.[13] found an inverse relationship between the CCT and axial length, which means that corneas are thinner in longer eyes. These results did not match our study.
Table 4 shows a comparison of our study results regarding the correlation of CCT with refractive errors with other published studies.
| Authors | Country | No of subjects | Subject recruitment | Equipment | CCT- Refractive errors relationship |
|---|---|---|---|---|---|
Von Bahr [25] |
Sweden |
125 |
General Ophthalmic Clinic |
Von Bahr's Apparatus |
Thinner in myopia less than -4D |
Nemesure.,et al. [29] |
Barbados |
1142 |
Barbados Eye Study |
USG |
Thicker in hypermetropia |
Pauline Cho.,et al. [27] |
United States |
35 |
Contact Lens Clinic |
Orbscan |
No correlation with hypermetropia |
Pederson., et al. [28] |
Denmark |
105 |
Refractive Surgery Clinic |
Optical |
No correlation |
H. Fam.,et al. [15] |
Singapore |
714 |
Refractive Surgery Clinic |
Orbscan |
No correlation |
A. Elias.,et al. [3] |
India |
203 |
General Ophthalmic Clinic |
USG |
No correlation with myopia |
This study |
India |
120 |
General Ophthalmic Clinic |
USG |
No correlation with myopia or hypermetropia |
Table 4:Comparisons of outcomes of other published studies with our study.
Our study's limitations are ultrasound pachymetry was done for measurement of central corneal thickness, which has a low reproducibility. We did not take diurnal variation of central corneal thickness, genetic and racial difference in CCT into consideration. There was a lack of very high myopes and not many hypermetropic subjects in the study. Purely astigmatic patients were excluded. Moreover, a larger sample size should be studied to further conclusively comment on the correlation of central corneal thickness with refractive errors and other variables.
We conclude that central corneal thickness has a negative correlation with corneal curvature, i.e., as the corneal curvature increases, the central corneal thickness decreases, and vice versa. However, there was no significant association between Central corneal thickness and other parameters like Age, Degree of Myopia, Hypermetropia, and Axial length.
I want to thank my mentor, colleagues, and our hospital's entire staff for their patience, guidance, and constant support throughout the study period.

Citation: Nair Shobita., et al. “Correlation of Central Corneal Thickness with Refractive Errors and Corneal Curvature in the South Indian Population". Acta Scientific Ophthalmology 4.4 (2021): 31-38.
Copyright: © 2021 Nair Shobita., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
