Immune Restoration Disorders in Patients with AIDS and Tuberculosis: Novel Treatment Approaches
Usha Kellampalli, Hesham Mohei and Irina Vlasova-St. Louis*
Division of Infectious Diseases and International Medicine, Department of Medicine, University of Minnesota, Minneapolis, MN, USA
*Corresponding Author: Irina Vlasova-St. Louis, Division of Infectious Diseases and International Medicine, Department of Medicine, University of Minnesota, Minneapolis, MN, USA.
Received: January 27, 2021; Published: February 20, 2021
Tuberculosis (TB) is the most frequent and treacherous opportunistic infection in patients with acquired immunodeficiency syndrome (AIDS) worldwide. In this review, we discuss the pathological immune restoration in AIDS patients coinfected with Mycobacterium Tuberculosis after starting ART (antiretroviral therapy). We overview how the immune deregulation predisposes to and drive the immune reconstitution inflammatory syndrome (TB-IRIS). We describe how poor recovery and maturation of T and NK cells, and the exuberant cytokine response produced by innate and adaptive immune cells marks the manifestations of TB-IRIS.
We conclude by discussing the various standard-of-care and novel treatment approaches.
Keywords: Immune Reconstitution Inflammatory Syndrome; Tuberculosis-IRIS; TB-IRIS; AIDS; HIV; Interferons; Cytokines; T Cell Response; Innate Immunity
Immune reconstitution inflammatory syndrome in AIDS patients co-infected with MTB
Tuberculosis (TB) is the most frequent and treacherous opportunistic infection in patients with acquired immunodeficiency syndrome (AIDS) worldwide.In late-stage HIV-infected patients, Tuberculosis (TB) is the most frequent opportunistic infection and is the major reason for morbidity and mortality, and TB-IRIS is a major clinical concern after ART initiation [1-3]. The leading manifestations of TB-IRIS are fever and exacerbating respiratory symptoms of miliary tuberculosis with worsening consolidations and pulmonary infiltrates [4,5].
Extrapulmonary TB-IRIS manifestations primarily include tuberculous meningitis, intracranial tuberculomas, or osteomyelitis [6,7]. The mortality and morbidity rates attributable to paradoxical TB-IRIS are elevated in settings where there are limited options for diagnosis and treatment [8-11].
The manifestations of TB-IRIS usually occur within 2-3 months of ART initiation or regimen change because of treatment failure [12,13]. The early-onset (< 1 month on ART) and late-onset (> 1 month on ART) TB-IRIS forms had been reported [14]. Recently proposed international network for the study of HIV-associated IRIS (INSHI) case definition system includes few radiographic imaging and immunological parameters with the proven diagnostic ability for either form of TB-IRIS. These include elevated levels of C-reactive protein (CRP), abnormal chest radiographs, and low pre-ART CD4+ T cell counts (< 100 cells/μl) [15]. Unfortunately, there is no laboratory diagnostics to definitively confirm TB-IRIS syndrome.
Kinetics of immune reconstitution in patients receiving antimicrobial and antiviral therapies
During Immune reconstitution, the kinetics of immune mediators
in blood and cerebrospinal fluid (CSF) demonstrated increased
levels of the innate pro-inflammatory cytokines IL1, IL6, IL8, and
TNFA (tumor necrosis factor alfa) in patients co-infected with HIV
and Mycobacterium tuberculosis (MTB) [16-18]. Before the beginning
of ART, there has been an increased level of IL6 and IL18 and
low levels of IL27, in patients at risk for TB-IRIS, and then followed
by the expansion of inflammatory monocyte subsets and inflammasome
activation during TB-IRIS events [19-23]. Cytokines such
as granulocyte-colony stimulating factor (GCSF), CRP, interleukins
IL1B, IL1RA, IL6, IL8, IL18, IFNG (interferon-gamma), TNFA, and
soluble tissue factors increased in plasma and serum after ART initiation
[24,25] (Figure 1). Along with these cytokines, the increases
of IL12p40, IL1β, GMCSF, TNF, IL10, IL6, IL2 and IL8 in serum and
in PBMC (peripheral blood monocyte cell) culture supernatants
render TB patients susceptible to TB-IRIS and early mortality
[20,26]. These parameters represent the baseline risk factors for
TB-IRIS, followed by the kinetic that is different from favorable cellular
immune reconstitution on ART and that, which accelerates
toward TB-IRIS event [27-29].
Recent genetic studies found the association of IRIS onset with KIR2DS2 (Killer Immunoglobulin-like Receptor, two Immunoglobulin Domains and Short cytoplasmic Tail 2), HLA-B*41, and KIR+/HLA-C genotypes among TB-HIV co-infected patients [30]. In patients at risk, NK/T cells have shown higher expression of the cytotoxic mediators (granzyme B and perforin) and certain effector T cell receptor subunits, which in turn amplifies the degranulation potential of effector T cells, creating a pro-inflammatory environment [31-33]. There has been a higher degranulation capacity of NK cells in patients with TB-IRIS before ART and after 2 weeks of TB treatment initiation, followed by lower expression of mature NK cell activating receptors (NKp30/p46, NK Group NKG2D) [28]. The expression of NKG2D (CD314+) on NK/T cells is lower in HIV-TB patients after ART initiation and the killer cell immunoglobulin like receptors (CD158a) expression was higher in TB-IRIS compared to non-IRIS patients before ART [34]. NK cells are activated during TB-IRIS events, and express higher readiness to migrate (CXCR1+, CXCR2+) in response to several pro-inflammatory mediators (C-reactive protein, IL8, etc.) [35].
During inflammation, MTB antigens and residual live mycobacteria activate toll-like receptor (TLR) signaling and inflammasome cascade, thereby causing notable damage to target cells and tissues [36-38]. Inflammasome, a multiprotein intracellular complex, is activated in macrophages, monocytes, and neutrophils and a role in systemic inflammation and fatal TB-IRIS outcomes [38-42]. Multiple elements of inflammasome activation occur via NLR- TREM1- pathways (NOD-like; and triggering receptor expressed on myeloid cells 1), representing exaggerated innate cells’ response toward ongoing viral replication and microbial antigens [43]. Studies have also found that the inflammasome pathway is a driver of CD4+ T cell depletion in HIV1-TB infection which delays immune reconstitution and serves as a biomarker of immune restoration pathology [44]. Thus, the inflammasome pathway overexpression in cells of the innate immune system represents a biomarker of systemic inflammation and significant pathology at the site of IRIS, e.g., the central nervous system in cases of TB-meningitis IRIS [21,45-47].
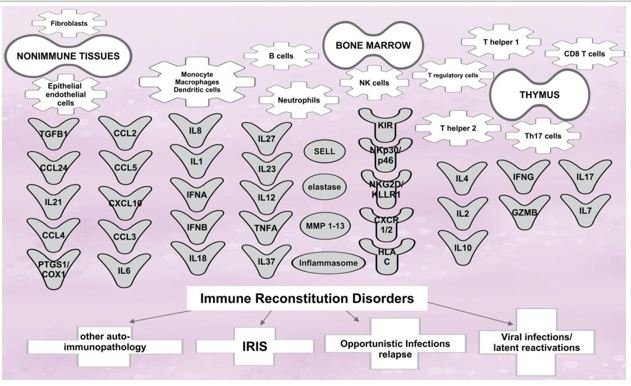
Figure 1: Cytokines, soluble factors, and cellular receptors, which play role in tuberculosisassociated immune reconstitution disorders.
In the early stages of immune restoration, CD4+, CD8+ T cells, NK/T cells express markers of lymphocytes exhaustion [48]. The expression of KLRG1 and PD-1 (programmed cell death 1) on CD4+ T cells and NK cells during recovery is similar in patients who developed TB-IRIS and survived, but low expression confers protection against MTB reactivation and over-exaggerated immune response to MTB antigens during IRIS [29,49,50]. Adaptive CD4+ T cells (together with CD8+ T cells) prompt to secrete higher amounts of IFNG and many other pro-inflammatory cytokines in response to TB antigens, which may lead to the over-exuberant cytokine response (Figure 1) [51,52]. This may particularly be attributable to early-onset forms of TB-IRIS since late-onset TB-IRIS patients showed a T cell maturation shift towards more mature T cell subtypes [14].
In the search for potential biomarkers, a recent study tested a
panel of seven anti-neutrophil cytoplasmic antibodies (ANCAs) in
the blood of patients who developed TB-IRIS after ART initiation.
Only one marker, an anti-elastase antibody found to be significantly
lower at ART initiation, and the other (anti-proteinase 3, anti-myeloperoxidase,
anti-bacterial permeability-increasing protein, anticathepsin,
-lysozyme, -lactoferrin) are not [53]. Taken into account
that expression of elastase increases at the time of TB-IRIS events
[41], exploration of anti-elastase as a potential therapeutic agent to
decrease neutrophils activation is plausible.
Novel and standard-of-care treatment approaches to counteract TB-IRIS
Since inflammatory responses discussed above are major drivers of TB-IRIS symptoms (Figure 1), the adjunctive corticosteroid therapy and co-trimoxazole prophylaxis has been associated with decreased inflammation and improved outcomes [54-56]. The use of prednisone is helpful to bring down acute symptoms in the short term in patients with TB-IRIS [57,58]. However, corticosteroids had shown to decrease the survival of T cells by augmenting apoptosis [59]. The addition of adjunctive treatment with IFNG, IFNA, or vitamin D supplementation, to prednisone therapy, has been useful to improve immune cell survival and decrease inflammation [60-63]. The serum concentration of cytokines such as IL10, IL12p40, IFNG, and chemokine CXCL10 decreased during 4 weeks of prednisone therapy [55].
The monoclonal antibody against IL6 has been reported to decrease severe forms of IRIS pathology in preclinical models [25]. Biologics such as adalimumab, infliximab, and other antiTNF agents like chloroquine or thalidomide can be useful if administered with ART to treat as well as to prevent TB-meningitis and TB-IRIS [63-65]. A combination of empirical doses of anti-TNF and corticosteroid treatment have been reported in recent literature as successful [66]. Other drugs such as pentoxifylline and hydroxychloroquine have been shown to be helpful in treating IRIS patients, with some reported benefits [67-69]. Other biologics such as Bevacizumab (anti-vascular endothelial growth factor, anti-VEGF) have been reported in the treatment of paradoxical worsening of TB-IRIS with retinal detachment [70]. Anakinra, a recombinant IL1 receptor antagonist, has been used as a therapeutic option for protracted paradoxical inflammation in HIV-associated TB IRIS [48].
In cases of steroid-refractory and leukotriene-driven inflammatory forms of TB-IRIS, treatment with Montelukast, a leukotriene antagonist, had shown prosperous outcomes [71,72]. Leukotrienes stimulate proinflammatory and antimicrobial properties by recruiting neutrophils to the sites of inflammation and increase immune responses [73,74]. Formal clinical trials need to be conducted to define the success of these therapies.
A randomized, double-blind, placebo-controlled clinical trial CADIRIS had assessed the effectiveness of CCR5 inhibitor Maraviroc. The inclusion of Maraviroc therapy into ART regimens (a combination of tenofovir, emtricitabine, and efavirenz) could not prevent TB-IRIS, thus did not confer meaningful protection [75].
Deregulation of innate and adaptive immunity (Figure 1) had
shown a primary role in the pathogenesis of immune reconstitution
inflammatory disorders [76,77]. Many pro-inflammatory mediators,
produced by natural killer (NK), intermediate NK/T, and
innate immune cells have been shown to take part in controlling
the immune responses during immune reconstitution.
As discussed above, a combination of abnormal frequencies of NK-cell receptor expression, high levels of IL6, IL10, TNFA, and IFNG, etc. represent the immune parameters that characterize TB-related IRIS. Thus, anti-inflammatory regimens that composed of corticosteroid therapy and several biologics may be clinically useful to manage TB-IRIS and improve patients’ outcomes.
The authors declare no conflict of interest.
This project was part of U01AI089244 (IV-S).
Not required.
- Török ME. “Tuberculous meningitis: advances in diagnosis and treatment”. British Medical Bulletin 113 (2015): 117-131.
- Wu Y., et al. “The prevention and control of tuberculosis: an analysis based on a tuberculosis dynamic model derived from the cases of Americans”. BMC Public Health 20 (2020): 1173.
- Suryana K. “A Challenge in Diagnosis of Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome (TB-IRIS)”. HIV AIDS (Auckl) 12 (2020): 263269.
- de Albuquerque YM., et al. “Chest radiographic findings in patients with HIV/AIDS and pulmonary tuberculosis”. International Journal of STD and AIDS 24 (2013): 951-956.
- Meintjes G., et al. “Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings”. Lancet Infection Disease 8 (2008): 516-523.
- Manosuthi W., et al. “Clinical case definition and manifestations of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome”. AIDS 23 (2009): 2467-2471.
- Bosamiya SS. “The immune reconstitution inflammatory syndrome”. Indian Journal of Dermatology 56 (2011): 476-479.
- Burman W., et al. “Frequency, severity and duration of immune reconstitution events in HIV-related tuberculosis”. International Journal of Tuberculosis and Lung Disease 11 (2007): 12821289.
- Lawn SD., et al. “Tuberculosis-associated immune reconstitution disease: incidence, risk factors and impact in an antiretroviral treatment service in South Africa”. AIDS 21 (2007): 335-341.
- Manosuthi W., et al. “Immune reconstitution inflammatory syndrome of tuberculosis among HIV-infected patients receiving antituberculous and antiretroviral therapy”. Journal of Infection 53 (2006): 357-363.
- Lawn SD., et al. “Immune reconstitution disease associated with mycobacterial infections in HIV-infected individuals receiving antiretrovirals”. Lancet Infection Disease 5 (2005): 361-373.
- Ali K and Klotz SA. “The immune reconstitution inflammatory syndrome with tuberculosis: a common problem in Ethiopian HIV-infected patients beginning antiretroviral therapy”. Journal of the International Association of Providers of AIDS Care 11 (2012): 198-202.
- Xue M., et al. “Prevalence and risk factors of paradoxical tuberculosis associated immune reconstitution inflammatory syndrome among HIV-infected patients in Beijing, China”. BMC Infectious Diseases 20 (2020): 554.
- Goovaerts O., et al. “Antigen-specific interferon-gamma responses and innate cytokine balance in TB-IRIS”. PLoS One 9 (2014): e113101.
- Stek C., et al. “Diagnostic accuracy of the INSHI consensus case definition for the diagnosis of paradoxical tuberculosis-IRIS”. Journal of Acquired Immune Deficiency Syndromes (2020).
- Bloom CI., et al. “Detectable changes in the blood transcriptome are present after two weeks of antituberculosis therapy”. PLoS One 7 (2012): e46191.
- Berry MP., et al. “An interferon-inducible neutrophil-driven blood transcriptional signature in human tuberculosis”. Nature 466 (2010): 973-977.
- Musselwhite LW., et al. “Vitamin D, D-dimer, Interferon gamma, and sCD14 Levels are Independently Associated with Immune Reconstitution Inflammatory Syndrome: A Prospective, International Study”. EBioMedicine 4 (2016): 115-123.
- Narendran G., et al. “Paradoxical tuberculosis immune reconstitution inflammatory syndrome (TB-IRIS) in HIV patients with culture confirmed pulmonary tuberculosis in India and the potential role of IL-6 in prediction”. PLoS One 8 (2013): e63541.
- Oliver BG., et al. “Mediators of innate and adaptive immune responses differentially affect immune restoration disease associated with Mycobacterium tuberculosis in HIV patients beginning antiretroviral therapy”. The Journal of Infectious Diseases 202 (2010): 1728-1737.
- Tan Y., et al. “Plasma interleukin18 levels are a biomarker of innate immune responses that predict and characterize tuberculosis-associated immune reconstitution inflammatory syndrome”. AIDS 29 (2015): 421-431.
- Tan HY., et al. “Aberrant Inflammasome Activation Characterizes Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome”. Journal of Immunology 196 (2016): 4052-4063.
- Andrade BB., et al. “Mycobacterial antigen driven activation of CD14++CD16- monocytes is a predictor of tuberculosis-associated immune reconstitution inflammatory syndrome”. PLoS Pathogens 10 (2014): e1004433.
- Grant PM., et al. “Elevated interleukin 8 and T-helper 1 and T-helper 17 cytokine levels prior to antiretroviral therapy in participants who developed immune reconstitution inflammatory syndrome during ACTG A5164”. The Journal of Infectious Diseases 206 (2012): 1715-1723.
- Barber DL., et al. “Role of IL-6 in Mycobacterium avium--associated immune reconstitution inflammatory syndrome”. Journal of Immunology 192 (2014): 676-682.
- Tadokera R., et al. “Hypercytokinaemia accompanies HIV-tuberculosis immune reconstitution inflammatory syndrome”. European Respiratory Journal 37 (2011): 1248-1259.
- Bourgarit A., et al. “Tuberculosis-associated immune restoration syndrome in HIV-1-infected patients involves tuberculin-specific CD4 Th1 cells and KIR-negative gammadelta T cells”. Journal of Immunology 183 (2009): 3915-3923.
- Pean P., et al. “Natural killer cell degranulation capacity predicts early onset of the immune reconstitution inflammatory syndrome (IRIS) in HIVinfected patients with tuberculosis”. Blood 119 (2012): 3315-3320.
- Haridas V., et al. “TB-IRIS, T-cell activation, and remodeling of the T-cell compartment in highly immunosuppressed HIV-infected patients with TB”. AIDS 29 (2015): 263-273.
- de Sá NBR., et al. “Clinical and genetic markers associated with tuberculosis, HIV-1 infection, and TB/HIV-immune reconstitution inflammatory syndrome outcomes”. BMC Infectious Diseases 20 (2020): 59.
- Johansson SE., et al. “NK cell function and antibodies mediating ADCC in HIV-1-infected viremic and controller patients”. Viral Immunology 24 (2011): 359-368.
- Walker NF., et al. “Invariant Natural Killer T cell dynamics in HIV associated tuberculosis”. Clinical Infectious Diseases (2019).
- Wilkinson KA., et al. “Cytotoxic mediators in paradoxical HIV-tuberculosis immune reconstitution inflammatory syndrome”. Journal of Immunology 194 (2015): 1748-1754.
- Pean P., et al. “High Activation of γδ T Cells and the γδ2”. Frontiers in Immunology 10 (2019): 2018.
- Cherif S., et al. “Unmasking immune reconstitution inflammatory syndrome: a report of tuberculous epididymo-orchitis mimicking a testicular tumour in a Caucasian AIDS patient”. International Journal of STD and AIDS 28 (2017): 100-103.
- Doitsh G., et al. “Cell death by pyroptosis drives CD4 Tcell depletion in HIV-1 infection”. Nature 505 (2014): 509-514.
- Mishra BB., et al. “Nitric oxide controls the immunopathology of tuberculosis by inhibiting NLRP3 inflammasome-dependent processing of IL-1β”. Nature Immunology 14 (2013): 52-60.
- Dorhoi A., et al. “Activation of the NLRP3 inflammasome by Mycobacterium tuberculosis is uncoupled from susceptibility to active tuberculosis”. European Journal of Immunology 42 (2012): 374-384.
- Diedrich CR and Flynn JL. “HIV-1/mycobacterium tuberculosis coinfection immunology: how does HIV-1 exacerbate tuberculosis?” Infection on Immune 79 (2011): 1407-1417.
- Tomlinson GS., et al. “HIV-1 infection of macrophages dysregulates innate immune responses to Mycobacterium tuberculosis by inhibition of interleukin-10”. The Journal of Infectious Diseases 209 (2014): 1055-1065.
- Nakiwala JK., et al. “Neutrophil Activation and Enhanced Release of Granule Products in HIV-TB Immune Reconstitution Inflammatory Syndrome”. Journal of Acquired Immune Deficiency Syndromes 77 (2018): 221229.
- Marais S., et al. “Neutrophil-associated central nervous system inflammation in tuberculous meningitis immune reconstitution inflammatory syndrome”. Clinical Infectious Diseases 59 (2014): 1638-1647.
- Lai RP., et al. “HIV-tuberculosis-associated immune reconstitution inflammatory syndrome is characterized by Toll-like receptor and inflammasome signalling”. Nature Communication 6 (2015): 8451.
- Tan HY., et al. “Aberrant Inflammasome Activation Characterizes Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome”. Journal of Immunology 196 (2016): 4052-4063.
- Marais S., et al. “Inflammasome activation underlies central nervous system deterioration in HIV associated tuberculosis”. The Journal of Infectious Diseases (2016).
- Tran HT., et al. “Modulation of the complement system in monocytes contributes to tuberculosisassociated immune reconstitution inflammatory syndrome”. AIDS (London, England) 27 (2013): 1725-1734.
- Tran HT., et al. “The role of monocytes in the development of Tuberculosis-associated Immune Reconstitution Inflammatory Syndrome”. Immunobiology 219 (2014): 37-44.
- Goovaerts O., et al. “Increased KLRG1 and PD-1 expression on CD8 T lymphocytes in TB-IRIS”. PLoS One 14 (2019): e0215991.
- Ravimohan S., et al. “Immunological profiling of tuberculosis-associated immune reconstitution inflammatory syndrome and nonimmune reconstitution inflammatory syndrome death in HIV-infected adults with pulmonary tuberculosis starting antiretroviral therapy: a prospective observational cohort study”. Lancet Infection Disease 15 (2015): 429-438.
- Verhofstede C., et al. “Correlation of coreceptor usage and disease progression. Current Opinion in HIV and AIDS 7 (2012): 432-439.
- Meintjes G., et al. “Type 1 helper T cells and FoxP3-positive T cells in HIV-tuberculosis-associated immune reconstitution inflammatory syndrome”. American Journal of Respiratory and Critical Care Medicine 178 (2008): 1083-1089.
- Ruhwald M., et al. “Immune reconstitution syndrome in tuberculosis and HIV-coinfected patients: Th1 explosion or cytokine storm?” AIDS 21 (2007): 882-884.
- Goovaerts O., et al. “Lack of elevated preART elastase-ANCA levels in patients developing TB-IRIS”. PLoS One 15 (2020): e0244800.
- Meintjes G., et al. “Management of active tuberculosis in adults with HIV”. Lancet HIV 6 (2019): e463-e474.
- Meintjes G., et al. “Corticosteroidmodulated immune activation in the tuberculosis immune reconstitution inflammatory syndrome”. American Journal of Respiratory and Critical Care Medicine 186 (2012): 369-377.
- Nunn AJ., et al. “Role of co-trimoxazole prophylaxis in reducing mortality in HIV infected adults being treated for tuberculosis: randomised clinical trial”. BMJ 337 (2008): a257.
- Meintjes G., et al. “Prednisone for the Prevention of Paradoxical Tuberculosis-Associated IRIS”. The New England Journal of Medicine 379 (2018): 1915-1925.
- Stek C., et al. “Preventing Paradoxical Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome in High-Risk Patients: Protocol of a Randomized Placebo-Controlled Trial of Prednisone (PredART Trial)”. JMIR Research Protocols 5 (2016): e173.
- Payne DN and Adcock IM. “Molecular mechanisms of corticosteroid actions”. Paediatric Respiratory Reviews 2 (2001): 145-150.
- Pappas PG., et al. “Recombinant interferon- gamma 1b as adjunctive therapy for AIDS-related acute cryptococcal meningitis”. The Journal of Infectious Diseases 189 (2004): 2185-2191.
- Jarvis JN., et al. “Adjunctive interferon-γ immunotherapy for the treatment of HIV-associated cryptococcal meningitis: a randomized controlled trial”. AIDS 26 (2012): 1105-1113.
- , et al. “Type I interferon: understanding its role in HIV pathogenesis and therapy”. Current of HIV/AIDS Report 12 (2015): 41-53.
- Lwin N., et al. “Adalimumab for Corticosteroid and Infliximab-Resistant Immune Reconstitution Inflammatory Syndrome in the Setting of TB/HIV Coinfection”. Open Forum Infectious Diseases 5 (2018): ofy027.
- Wallis RS., et al. “Adalimumab treatment of life-threatening tuberculosis”. Clinical Infectious Diseases 48 (2009): 1429-1432.
- Hsu DC., et al. “A Paradoxical Treatment for a Paradoxical Condition: Infliximab Use in Three Cases of Mycobacterial IRIS”. Clinical Infectious Diseases 62 (2016): 258-261.
- Nabeya D., et al. “Use of steroids to treat anti-tumor necrosis factor α induced tuberculosis-associated immune reconstitution inflammatory syndrome: Case report and literature review”. Medicine (Baltimore) 99 (2020): e22076.
- Bell HC., et al. “Pulmonary Mycobacterium celatum immune restoration disease: immunopathology and response to corticosteroid therapy”. AIDS 19 (2005): 2047-2049.
- Wallis RS., et al. “Pentoxifylline in human immunodeficiency virus- positive tuberculosis: safety at 4 years”. The Journal of Infectious Diseases 178 (1998): 1861.
- John M and French MA. “Exacerbation of the inflammatory response to Mycobacterium tuberculosis after antiretroviral therapy’. Medical Journal of Australia 169 (1998): 473-474.
- Jain S., et al. “Bevacizumab for paradoxical worsening treatment adjunct in HIV patient with choroidal tuberculoma”. Journal of Ophthalmic Inflammation and Infection 6 (2016): 42.
- Hardwick C., et al. “Montelukast in the treatment of HIV associated immune reconstitution disease”. Sexually Transmitted Infections 82 (2006): 513-514.
- Lipman MC and Carding SK. “Successful drug treatment of immune reconstitution disease with the leukotriene receptor antagonist, montelukast: a clue to pathogenesis?” AIDS 21 (2007): 383-384.
- Coffey MJ., et al. “Granulocyte colony-stimulating factor administration to HIV-infected subjects augments reduced leukotriene synthesis and anticryptococcal activity in neutrophils”. Journal of Clinical Investigation 102 (1998): 663-670.
- Peters-Golden M., et al. “Leukotrienes: underappreciated mediators of innate immune responses”. Journal of Immunology 174 (2005): 589-594.
- Sierra-Mader JG., et al. “A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of a Chemokine Receptor 5 (CCR5) Antagonist to Decrease the Occurrence of Immune Reconstitution Inflammatory Syndrome in HIV-Infection: The CADIRIS Study”. Lancet HIV 1 (2014): e60-e67.
- Mohei H., et al. “Immune Reconstitution Disorders: Spotlight on Interferons”. International Journal of Biomedical Investigation 2 (2019).
- Kellampalli U., et al. “Kinetics of immune reconstitution and immune complications after cell and organ transplantation”. Integrative Cancer Science and Therapeutics 7 (2020): 1-6.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License