Sunita Singh1, Chandrashekharaiah PS1, Vishal Paul1, Santosh Kodgire1, Shivbachan Kushwaha1, Debanjan Sanyal1* and Santanu Dasgupta2
1Reliance Industries Ltd, Jamnagar, India
2Reliance Industries Ltd, Reliance Corporate Park, Ghansoli, India
*Corresponding Author: Debanjan Sanyal, Reliance Industries Ltd, Jamnagar, India.
Received: January 18, 2021; Published: February 20, 2021
Citation: Sunita Singh., et al. “Human Immune Response to COVID-19 Infection and Potential Role of Chloroquine Family of Drugs: A Review”. Acta Scientific Microbiology 4.3 (2021): 104-118.
In December 2019, COVID-19 disease outbreak started from Wuhan, China. World is still, witnessing a massive morbidity and mortality due to the pandemic caused by novel coronavirus severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2). This newly discovered virus enters inside and infect the body cells through the angiotensin-converting enzyme 2 (ACE2) receptor. The S1 protein of SARS-CoV-2 binds to the ACE2 receptor which results in endocytosis and transfer of virus into endosomes of body cells. Entry of SARS-CoV-2 results in activation of the innate immune responses first followed by the adaptive immune responses. The effective host immune responses are crucial to control and prevent the viral infections. However, the excessive production of proinflammatory cytokines and decrease in the number of T-lymphocytes are the major reasons associated with severity of COVID-19. Therefore, anti-inflammatory drugs such as Chloroquine (CQ) and hydroxychloroquine (HCQ) may play a crucial role to control and prevent the progression of disease by immunomodulation. The treatment responses of COVID-19 patients to these drugs have been found positive in some cases and clinical studies are underway for evaluating these drugs for the same. Moreover, regulatory bodies such as Food and Drug Administration (FDA) and European Medicines Agency (EMA) have recommended usage these drugs in emergency and chronic situation to treat critically ill COVID-19 patients under doctor’s supervision. The national task force (NTF) set up by Indian Council of Medical Research, has recommended high risk individuals to take HCQ for prophylaxis. This review summarizes human immune response and various aspects of CQ and HCQ with special reference to COVID-19.
Keywords: Chloroquine; COVID-19; Hydroxychloroquine; Immune Response; SARS-CoV-2
The SARS-CoV-2 belongs to β-coronavirus family and is responsible for causing COVID-19 disease which mainly attacks human respiratory system [1]. This disease is primarily transmitted through the respiratory droplets of infected person while coughing and sneezing. Secondly, the virus gets into mouth, nose and eyes when someone is in close contact with COVID-19 infected person. Also, this virus can remain stable on the inanimate surfaces for many hours or even days. Touching these surfaces with subsequent touching of mouth, nose, eyes, may also lead to transmission of the disease. The incubation period for this virus varies from 1 to 14 days, however, it was found to spread even during the dormant period [2]. The cough and fever are the most common symptoms of this disease and in severe cases, lung inflammation, acute respiratory distress syndrome (ARDS), cardiac and renal injuries were also observed. The pre-symptomatic and asymptomatic carriers have become the main reason for human to human transmission and rapid spread of the disease across the world [3]. Originating from Wuhan, China, till date, this pandemic has spread in >212 countries and territories around the world. Total number of confirmed COVID-19 cases reported as on 20th July, 2020 are >14million and death toll has reached to >6 lakhs, globally. The frequency of COVID-19 occurrence is higher in elderly people, with compromised immune system and the people who are having diabetes and cardiovascular diseases. The SARS-CoV-2 virus takes entry into body through ACE2 receptors and establish the infection process [4]. T lymphocytes are the major target cells for the virus. In severe COVID-19 cases, drastic reduction in number of natural killer (NK) cells, CD4 and CD8 T lymphocytes and excessive production of cytokines was observed which lead to immune dysfunctioning. Until now, there is no proven or registered drug for COVID-19. The increased death rate and rapid spread of the disease across the world has created the global emergency and made medical professionals, policy makers to explore all possible, potential treatment strategies to control and eliminate the outbreak.
Based on the current understanding about virus pathophysiology and the symptoms of the disease, specific drugs with antiviral and immunomodulatory properties will be ideal to control the disease. However, several clinical trials are in progress to test antiviral, immunosuppressive or immunomodulatory drugs against COVID-19 [5]. The previous experience of handling the diseases caused by viruses belonging to the β-coronavirus family such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) causing pneumonia has provided some background for designing the treatment strategy for COVID-19. Anti-malarial drug CQ and its less toxic derivative HCQ, are well known agents for immunomodulation and are being used in rheumatology. For many years, these drugs have been used to treat autoimmune disease like systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA). During the outbreak of SARS corona virus, CQ was used in some cases as an antiviral agent to control the infection [6]. Many recent studies have suggested the use of these antimalarial drugs to control the COVID-19 infection and several clinical trials are under way [7]. This review summarizes the pathogenesis of SARS-CoV-2, general human immune responses, specific immune responses against COVID-19, mode of action and possible treatment by CQ and HCQ and global regulatory perspective on usage of these drugs.
Structure of SARS-CoV-2 and Its PathogenesisCoronaviruses are pleomorphic, positive stranded RNA viruses (26-32 kb) having 80-120 nm diameter. These viruses have been classified in to four type’s α-COV, β-COV, δ-COV and γ-COV. The newly identified SARS-CoV-2 coronaviruses belongs to β-coronavirus type. All these viruses are known to cause respiratory diseases in human beings [8]. The genome of SARS-CoV-2 encodes 4 structural proteins; Nucleocapsid (N), Membrane (M), Envelope (E) and Spike (S) with various accessory proteins as well [2]. The nucleocapsid or N-protein coats and the viral RNA genome which plays a vital role in its replication and transcription. The M-protein is abundantly present on the viral surface and it is believed to be the central organizer for coronavirus assembly [9]. The E-protein is a small membrane protein which plays an important role in virus assembly and interaction of virus with host cell [10]. The process of infection mainly starts with the interaction of coronavirus S protein with the corresponding ACE2 receptor present on the target cell. After recognition and attachment of coronavirus, it injects its RNA in to target cell by protease cleaving and membrane fusion [11]. Once RNA enters in to host cell the replication and transcription of viral RNA are mediated by replication/transcription complex (RTC) [12]. Subsequently the viral envelope glycoproteins are synthesized in the cytoplasm and then viral assembly is established inside the endoplasmic reticulum (ER). Viral assembly formed by the combination of genomic RNA and nucleocapsid protein in the Endoplasmic Reticulum-Golgi Intermediate Compartment (ERGIC). After the formation of virions assembly, these are transported from Golgi vesicles and ultimately released by exocytosis so that they can infect other healthy cells.
The S protein of SARS-CoV-2 plays a major role in initiating the infection [13]. S protein of SARS-CoV-2 also has an affinity to bind with host cellular transmembrane serine protease (TMPRSS). Considering the higher affinity to ACE2 and TMPRSS, these can be considered as potential targets for developing drug to control SARS-CoV-2. Presence of furin-like cleavage site was reported on S protein of SARS-CoV-2, that is believed to be cleaved by furin convertase, for improving the fusion of viral particle with host cell membrane [14]. Apart from this, another furin type recognition site named “RRAR” has also been found in S1/S2 cleavage site of SARS-CoV-2. Also, by molecular modelling a new site on S protein of SARS-CoV-2 was identified at N-terminal domain (NTD) called as gangliosides binding domain [15]. This site of virus is required for attachment to lipid rafts and ACE2 receptors by binding to sialic acids (N-Acetylneuraminic acid) which is connected to host cell surface gangliosides. The mechanism of recognition and attachment of SARS-CoV-2 is considered to be similar as like SARS-CoV.
Although the mechanism of pathogenesis of SARS-CoV-2 is not well understood completely, a probable cellular response is being assumed based on earlier research on SARS-CoV. In an initial 1-2 days of infection virus binds to ACE2 receptor of epithelial cells with a limited innate immune response and this stage of infection can be labelled as asymptomatic state [16]. In next stage of infection (7-14 days) virus travels down the respiratory tract and elicits strong innate immune response. The level of cytokines such as CXCL10, lambda and beta interferon get increased in viral infected cells. In third stage of infection virus cause severe disease by infecting lung alveolar type II cells. In third stage the virus mainly damages alveolar cells with fibrin rich hyaline membranes which leads to the formation of multinucleated giant cells.
Till date, there are significant gaps in understanding the pathogenesis and human immune response of this virus. Therefore, it’s crucial to explore the reasons of failure of immune response in COVID-19 patients. An extensive knowledge and clinical findings about human immune responses against SARS-CoV-2 infection would play a critical role in designing an appropriate therapeutic approach to combat COVID 19 pandemic.
General immune responseImmune response is a reaction that occurs in response to the foreign invaders inside the human body. It protects the body from the disease causing organisms such as, bacteria, viruses and other substances. As microbes are omnipresent therefore, human beings are exposed to millions of potential pathogenic microbes which may enter through contact, ingestion and inhalation. These microbes contain a wide range of toxic or allergenic substances which are threat to normal physiology of humans and other mammals. Pathogenic microorganisms such as bacteria and viruses possess various mechanisms by which they infect the host organisms. Mostly, pathogens penetrate through the primary barriers, enter and multiply in extracellular spaces inside the body of host organism while the intracellular pathogens such as viruses spread via extracellular fluids. This lead to alteration in normal body functioning and hence disease occurs. At the same time, immune system recognizes these pathogens as non-self or foreign elements and tries to destroy substances that contain antigen. A general feature of the immune system is to detect structural features of the pathogen or toxin that mark it as distinct from the host cells. To minimize the risk of infection without harming its own tissues, the discrimination between host and pathogen is very crucial. In human beings, immune response is an extremely sophisticated that involves both innate and adaptive response. These responses consist of network of many cells and organs that work synergistically to protect the body against foreign invaders [17]. The cellular components involved in immune response are predominantly produced by bone marrow, which serves both the hematopoietic and immunopoietic functions. Bone marrow, a lymphoid tissue is of paramount importance in most of mammalian species. It acts as both primary and secondary lymphoid organ to regulate the production, differentiation and maturation of lymphocytes [18].
Innate immune responseInnate immune responses are nonspecific and rapid responses which are activated by the receptors that are encoded by genes present in the germ line of host organism. Innate responses comprise of physical, chemical and cellular barriers that form the first line of defence against pathogenic microbes. Physicochemical barriers mainly include skin, mucus membranes, tears, cough reflexes and stomach acids. While the chemical barriers include soluble proteins, cytokines, chemokines, complement proteins, defensins and ficolins [18]. The cellular barriers involved in innate immune response comprise of numerous cells such as phagocytes (macrophages and neutrophils), dendritic cells, mast cells, basophils, eosinophils, natural killer (NK) cells and innate lymphoid cells (Table 1) which help in impeding the infections [19]. The main purpose of the innate immune response is to straightaway prevent the spread of foreign pathogens throughout the body. Penetration of pathogen inside the body of host lead to activation of myeloid and mononuclear phagocytes. These cells react to the chemotactic factors released by either affected cells or by pathogen itself and abolish the pathogens quickly via phagocytosis. The cellular elements of innate immune responses unable to recognize the epitopes present on an antigen as precisely as observed in adaptive immune responses. Therefore, these responses to pathogen profoundly relies on the interaction of cell surface receptors known as pattern recognition receptors (PRRs). These receptors permit specific immune cells to identify and respond quickly to an extensive range of pathogens that share common structures with them, such common structures are known as pathogen-associated molecular patterns (PAMPs) [20]. Natural antibodies, the complement receptors, mannan binding proteins, lipopolysaccharides (LPS), the cell wall components of bacteria and double stranded RNA that is produced during any viral infections are examples of PAMPs [20]. Innate immune responses also consist of soluble factors such as serum proteins. These proteins bind to the surface of invading pathogens and are referred as opsonins. Opsonins make the pathogens more susceptible to engulfment by the immune cells via the process of phagocytosis. Likewise, cytokines and chemokines are small proteins secreted by the immune cells at site of infection and inflammation. These proteins help in cell signalling and activation of the local cellular immune responses at infection site as well as activate many defence mechanisms throughout the body. The main inflammatory cytokines released during early immune response to pathogen infection consist of tumour necrosis factor (TNF), interleukin 1 (IL-1) and interleukin 6 (IL-6). These cytokines are crucial for initiating the immune cells mobilization, the local inflammation and development of fever which is required for clearance of pathogens. Additionally, these cells help in processing and presentation of antigen during specific immune responses, intensification and control of immune responses by the release of soluble interleukin mediators. Simultaneously, these cells also help in removal of dead and broken cells which is very crucial for the healing process. Innate immune responses activate adaptive immune responses via activation of antigen-presenting cells (APCs) [21].
Adaptive immune responseAdaptive immune responses are acquired responses that are specific in nature and act as second line of defence. Contrary to germinal encoded recognition molecules of innate immune response, the adaptive responses are encoded by gene elements that somatically rearrange to assemble antigen- binding molecules with exquisite specificity for individual unique foreign structures. The main characteristic feature of adaptive immune response is rapid multiplication and increase of T and B lymphocytes from one or a few cells to millions against an infection. Adaptive responses are primarily based on the antigen-specific receptors expressed on the surfaces of T and B lymphocytes [22]. Key features of adaptive immune response are; specificity and the range of recognition, memory, specialized response, self-restraint and tolerance to components of the organism. The essential components of acquired immune response are T and B lymphocytes, immunoglobulins (antibodies) and antigen presenting cells (APCs) (Table 1) [22]. APC’s plays a key role in activation of naive T- cells via major histocompatibility complex (MHC) molecules on cell surface. Antigen presenting cells includes dendritic cells, B-cells and macrophages which are equipped with MHC molecules and co-stimulatory ligands which are predicted by stimulatory receptors present on helper T-cells [18]. When innate immune response become ineffective against growth of microbes, specific immune response gets triggered against the epitopes of pathogen by an interaction with major histocompatibility complexes I /II interleukins (IL), and T-lymphocytes (TH and TC) [18]. The cells produced during adaptive immune response are long lived and remain seemingly in dormant state, however, these cells can re-express their functions swiftly after repetitive encounter with their specific antigen [20]. This results in manifestation of immune memory and make the adaptive immune response more effective against specific pathogens or toxins. As adaptive immune response is specific and meant to attack pathogens but can sometimes it may make mistakes in recognizing the structure of pathogen and attack itself. The capability of the immune response to prevent self-damage is known as self-tolerance and failure of self-tolerance triggers the broad class of autoimmune diseases like lupus and rheumatoid arthritis. The innate and adaptive immune responses usually act together. To combat against any pathogen, the synergy between both the immune responses is crucial for an intact, fully effective immune response. In many cases, early induced responses were found not so effective in controlling the pathogen growth. However, these responses slow down the growth of pathogens and hence, allow time for strengthening of the adaptive immune response to control or eliminate the pathogen [23]. Adaptive immune response is further classified into the cell-mediated immune response, which is carried out by T cells, and the humoral immune response, that is controlled by activated B cells and antibodies. Activated T cells and B cells that are specific in nature and recognise the molecular structures present on the pathogen. These cells kill pathogens directly by apoptosis or by secreting antibodies which results in enhancing the process of phagocytosis and disrupt the infection [24].
Cell mediated immune response/T-cell mediated immune responseCell mediated immune responses are critical in maintaining the normal homeostasis of an individual. These responses are function of T lymphocytes leading to production of effector T-cells. T lymphocyte originates from bone marrow, matures in thymus gland, and play a vital role in immune response. There are four different types of T cells: helper, cytotoxic, memory and regulatory T cells. Helper T cells help in maturation of B cells and activation of cytotoxic T cells and macrophages via interleukin; cytotoxic T cells or killer T cells destroy virus-infected cells and tumour cells in the cell-mediated immune response. Similar to B cells, T cells are antigen specific cells that get converted to effector T cells and provides rapid response when re-exposed to specific pathogen to previous infection. T cells and B cells are deactivated by regulatory or suppressor T cells whenever needed to prevent the immune response from becoming too intense [25]. T-cells recognize the antigens based on a two-chain protein receptor. Mainly, APCs (antigen presenting cells) enzymatically cleaves the antigen into smaller fragments and bring them to cell’s surface. These fragments with a specific type of antigen-presenting protein is known as a MHC molecule. Association of the antigen fragments with an MHC molecule on the surface in the recognition of antigen by a T cell. Antigens from different types of pathogens use different class of MHC molecules that is MHC-I and MHC-II. However, these molecules bring processed antigen to cell’s surface through a transport vesicle and present the antigen to the T cell receptor. Immature T cells can express either CD4 (cluster of differentiation 4) or CD8 molecules on their cell surface. These molecules primarily regulate the interaction of T-cell and APC. CD4 cells bind APCs via antigen embedded MHC II molecules and stimulate to form helper T-cells. Helper T-cells further stimulate B-cells or cytotoxic T cells directly or secrete cytokines such as interferons (IFN)-gamma and interleukin to inform target cells about pathogenic threat [26]. CD8 bearing T cells are associated with cytotoxicity as CD8 molecules interacts with an intracellular pathogen and engage antigen embedded MHC I molecule on APCs. These cells are stimulated to become cytotoxic T-cells (CTLs) which kill the infected cells directly by apoptosis and release cytokines to intensify immune response. During an intense immune response there is rapid increase in cytotoxic T cell production and hence these cells kill the virus infected cells before completion of virus replication cycle. Due to effective antiviral immune response of cytotoxic T-cells, adaptive/active immune response has been evolved at first place.
Humoral immune response/B-cell mediated immune responseHumoral immune response is a function of B-cells and originates in bone marrow, hence it is known as B-cell or antibody mediated response [18]. Like T-cells, B-cells carry antigenic surface receptors known as CD antigens (cluster of differentiation). Till date, more than 80 CD antigens have been reported in mammals. Mostly, B cells carry both MHC I and MHC II class antigens, complement receptors, several interleukin receptors and discrete B-cell receptor which is capable to bind with APC processed or free antigen [18]. B cells are stimulated by helper T-cells and are differentiated into plasma cells or memory cells. Plasma cells are the immune cells which secrete large amount of antibodies or immunoglobulins. These are specialized glycoproteins responsible to neutralize the invading pathogens by recognizing the antigen present on cell surface via fragment antigen binding (FAB) variable region and cause phagocytosis [27]. In human beings, five different classes of antibodies have been identified: IgM, IgD, IgG, IgA and IgE. Amongst these five classes of immunoglobulins, only IgM and IgD function as antigen receptor for naive B cells. Immune responses are triggered by entry of the foreign elements in body called antigens and are classified into primary and secondary immune responses [20]. The initial encounter of immature B cells to an antigen induces primary immune response. Depending on type of antigen and site of infection primary immune response may take up to 14 days to resolve and leads to generation of memory B cells with a higher specificity against antigen. IgM is mostly stimulated by the primary immune response, however, IgG participates in for the memory response [28]. Any kind of subsequent exposure to same antigen lead to the development of secondary immunological response which increases the magnitude of the immune response by production of antibodies at much faster rate. During secondary immune response memory T cells quickly multiply into helper T cells and cytotoxic T cells while memory B cells produces antibodies to counteract the pathogen. Unlike T cells, B cells can recognize innate antigen and hence these cells do not entail participation of MHC molecules and antigen-presenting cells. Most protein antigens require signals from helper T cells (Th2) or interleukin to make antibodies. Th2 cells provide help to B cells in controlling extracellular pathogens and are essential for antibody mediated immune response. The specific receptors present in B cells bind to soluble antigens and engulf them via receptor-mediated endocytosis. Th2 cells with complementary T cell receptors (TCRs) bind with B cells and secrete lymphokines or interleukin which induce B cell differentiation to produce plasma cells. Antibodies produced by B cells destroy the pathogens in extracellular spaces and thus prevent spread of intracellular infection. When B cell binds to a self-antigen, in absence of signal from nearby T helper cells to produce antibody, the cell is summoned to undergo apoptosis and destroyed. The B cells after destroying the antigens, produce memory cells which in turn provide future immunity when the same antigen triggers inside body again.
|
Immune Response |
Type of cells |
Primary Location |
Target Pathogens |
Function |
References |
|
|
Type |
||||||
|
Innate |
Macrophages |
Body cavities and organs |
Broad range (Bacteria, viruses, protozoans) |
Phagocytosis and antigen presentation to T cells |
[29] |
|
|
Neutrophils |
Blood |
Bacteria and Fungi |
Phagocytosis and degranulation (discharge of contents of cells) |
[30] |
||
|
Eosinophils |
Blood |
Parasites and allergic tissues |
Degranulation, Release of enzymes, growth factors, and cytokines |
[31] |
||
|
Basophils |
Blood |
Various allergic tissues |
Degranulation, Release histamines, enzymes, growth factors and cytokines |
[19] |
||
|
Mast cells |
Connective tissues, gastrointestinal tract, skin and respiratory epithelium |
Parasites and various allergic tissues |
||||
|
Lymphocytes/ T-cells |
Thymus and lymph nodes |
Th cells target intracellular bacteria, Cytotoxic T cells target virus infected and tumour cells |
T helper (Th) cells, (CD4+): immune response mediators, Cytotoxic T cells (CD8+): Release of cytokines, perforin and granzymes which induce apoptosis |
[32] |
||
|
Monocytes |
Blood |
Various microbes |
Precursor of mast cells and dendritic cells, Differentiate into macrophages and dendritic cells to elicit an immune response |
[33] |
||
|
Natural Killer Cells (NK) |
Blood, body cavities and tissues |
Viruses and Tumour cells |
Tumour rejection, Destruction of infected cells, Release of perforin and granzymes which induce apoptosis |
[34] |
||
|
Adaptive |
T-Cells |
Th -Cell |
Formed in bone marrow and maturation in Thymus, lymphoid tissues |
Bacteria and Viruses |
T helper (Th) cells, (CD4+): immune response mediators, Cytotoxic T cells (CD8+): cell destruction |
[35] |
|
TC- Cell |
||||||
|
Treg- Cell |
||||||
|
B-Cells |
Memory B-Cells |
Formation and maturation in bone marrow, lymphoid tissues |
Bacteria and Viruses |
Linear and conformational epitopes on virions and virus infected cells, releases mediator molecules immunoglobulins (Ig) |
[[36] |
|
|
Plasma B-Cells |
||||||
Table 1: Cellular components/elements involved in human immune responses (Th: Helper T cell, Tc: Cytotoxic T cell, Treg: Regulatory T cell, CD4+: Cluster of differentiation 4: CD8+: Cluster of differentiation 8).
Immune response against COVID-19Clinically, in response to COVID-19 infection, both innate and adaptive immune responses get triggered to kill the virus and protect the body against infection. Immune responses vary at different stages of infection. Previous studies on SARS coronavirus revealed that this virus predominantly targets airway epithelial cells, alveolar epithelial cells, vascular endothelial cells, and macrophages in the lungs. All these cells express the ACE2 host target receptor and the same is being used by SARS-CoV-2 at the entry point, hence these cell subsets are specifically targeted by this virus [37]. Once the virus interrupts primary protective barrier it hijacks host cell machinery and increase their number by rapid multiplication. This leads to huge damage to affected tissues particularly in the organs with high ACE2 expression, such as kidney, liver, and intestine. These damaged cells and tissues may further lead to hyper-activation of innate response (monocytes and macrophages) that causes hyper inflammation in the lungs (fig.1). Therefore, in COVID-19, immune hyperactivity is reported to be the main cause of acute lung injury and ARDS at a severe stage. It has also been reported that tissue-resident macrophages in the lungs were found to be associated with epithelial damage which leads to the initiation of ARDS [38]. The macrophages are stimulated by heat shock proteins or intracellular hyaluronan fragments released by injured cells and PAMPs such as viral RNA or oxidized phospholipids. Molecules from damage-associated molecular patterns (DAMPs) and PAMPs trigger multiple innate immune responses through TLRs (toll-like receptors), NLRP3 (Nod-like receptor protein)/inflammasome activation. Signal transduction by these molecules initiates the production of cytokines and chemokines such as IL-6, IFNγ that activates antiviral gene expression in neighbouring cells and deploy additional innate and adaptive immune cells to counteract viral infection and maintain tissue homeostasis [39]. The production of IFN types I and III leads to activate neighbouring epithelial cells with intracellular antiviral defence, which further reduce the dissemination of viral particles. Whereas, the release of IL-6 and IL-1β by monocytes triggers the mobilization of neutrophils and cytotoxic T cells [39]. Activated neutrophils release ROS (reactive oxygen species) and leukotrienes that induces endothelial damage, which leads to severe lung destruction. However, IL-6 promotes the maturation of T helper cells as well as naive B cells for antibody production to ensure long-term immunity. Further, by recruiting additional immune cells IL-6 amplifies innate immune responses [40]. In contrast to this, IL-1β got cleaved in response to inflammasome activation and act locally in improving neutrophil cytotoxicity. Available data indicates that enhanced production of cytokines and chemokines create imbalance and dysregulation of the innate immune response which becomes the main cause of the severity of the infection. Such elevations in innate immune cytokines are also known as “cytokine storm,” these are similar to the cytokine release syndrome (CRS) which is accountable for cell toxicity and multiple organ impairment mediated by COVID-19 infections. Irrespective of clinical evidence about dysregulation of innate immune responses is a cause of COVID-19 morbidity and mortality, it is very much clear that viral transmission is a key driver of the deadly disease. The histopathologic study performed by clinicians on specimens collected from severely affected COVID-19 patients revealed the presence of inclusion bodies with viral persistence [40]. The consistent viral persistence may be due to inadequate activation of type I and type III interferons, which lead to failure of the innate immune response.
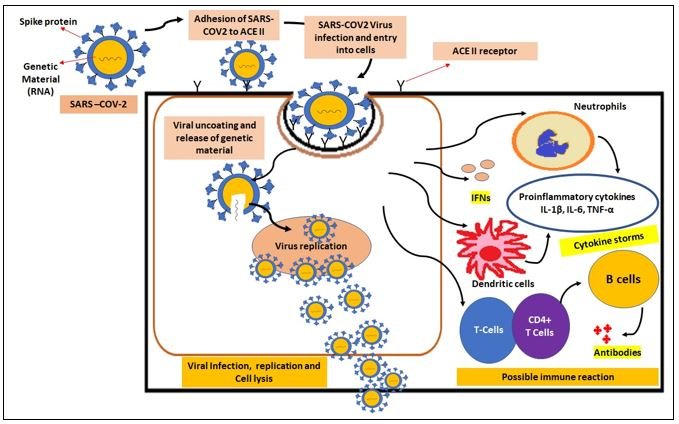
Figure 1: SARS –COV-2 infection and Immune reaction. Viruses enters healthy cells through ACE II receptors.
In the cytoplasm, the virus releases genetic material (RNA), replicates rapidly, and damages host tissue by exocytosis. Infected cells produce interferons (IFNs) against the virus as a primary immune reaction. Once these IFNs were dampened by the virus, the incoming neutrophils, dendritic cells produce the cytokine storms. The B cells activated by CD4+ T cells produce specific antibodies to inactivate the virus.
Research in immunology has established the fact that to clear and maintain long term suppression of viral infections, activation of T-cell mediated adaptive immune responses are very much needed. T lymphocytes play a vital role in antiviral responses against SARS-CoV-2. One week after the beginning of COVID-19 symptoms, the presence of both B-cells and T-cells has been detected in the blood samples against SARS-CoV-2. During acute viral infections, the viral peptides activate naive CD4+T cells and CD8+T cells proliferation. CD8+T cells play a significant role in directly killing the virus infected cells, whereas, CD4+T cells are crucial for enhancing CD8+T cell and B cell immune responses [41]. Also, CD4+ T cells are responsible for the production of cytokine for immune cell recruitment. Autopsy of a patient infected with COVID-19 showed accumulation of mononuclear cells such as monocytes and T cells in the lungs. Whereas presence of low levels of reactive T cells was found in peripheral blood, this state of a reduced level of lymphocytes is also known as lymphopenia or lymphocytopenia. Studies suggest the reason behind the decreased levels of T cells (CD4+ and CD8+) in peripheral blood is their movement away from blood and mobilization towards the site of infection to kill the infected cells and to prevent the viral dissemination. Amplified exhaustion of T cells or depleted lymphocytes (PLD) contributes to severe outcomes such as viral persistence and mortality in COVID-19 infected patients [42]. However, in the case of well-regulated adaptive T cell-mediated response and improvement in T cell count both CD4+ and CD8+ directly lead to clinical recovery [40]. Patients recovered from COVID-19 infection shown signs of clonal expansion, T cell activation, and memory T cell formation.
The humoral immune response is a main component of memory response, which plays an important role in virus clearance and prevents its reoccurrence. B cell-mediated responses act concurrently with T helper cell responses [43]. According to studies, robust B cell responses have been prompted by SARS-CoV-2 virus, which is supported by the presence of virus-specific immunoglobulins such as IgG, IgM, IgA, and neutralizing IgG (nAb). Stimulated B cells lead to the production of antibodies that respond to the spiked protein within 2-8 days of onset of symptoms against COVID-19 and immunoglobulins IgM are the first antibodies that appear in response to an infection followed by IgG. In most COVID-19 cases seroconversion takes place between 7 to 14 days of onset of symptoms and antibody titres persist for 2-3 weeks or even more than that following the clearance of the cytopathic virus [44]. Primarily, the immunoglobulins (IgG and IgM) bind to the SARS-CoV-2 internal N protein as well as with the S glycoprotein receptor-binding domain (S-RBD) that is present externally [45]. The antibodies binding with the S-RBD domain can trigger the immune responses further and this may lead to neutralize or block the virus interactions with the host entry receptor, ACE2 [45]. In most of the blood samples of COVID-19 cases, the presence of virus-specific antibodies (IgG, IgM, IgA, and anti- RBD nAbs) were detected even after 50 days of recovery [45]. Thus, specific immunoglobulins IgG and IgM can serve as an immunological marker against COVID-19 and serve as an early detection tool to identify COVID-19 infected host/patient. As the severity of COVID-19 is linked with enhanced IgG response, this could serve as a complementary tool to distinguish between mild and severe COVID-19 cases. Also, therapeutic approaches to modulate the immunity can be strategized based on both T cell and B cell-mediated responses.
In malaria and COVID-19 disease conditions, initially innate immune response and later on adaptive immune response are produced. In both the diseases, Th cells CD4+ and CD8+ play a vital role in pathogen removal by phagocytosis. Decreased levels of T lymphocytes and increased cytokine production contributes to severe pathogenic infection of COVID-19. Since, CQ/HCQ are the approved drugs that have been used previously for the treatment of diseases related to ARDS, autoimmune disorders, and hyper inflammation. Therefore, in the current situation, the immunomodulatory and anti-inflammatory drugs CQ/HCQ may prove effective in controlling COVID-19.
General use of CQ/HCQ and mechanism of actionHydroxychloroquine (HCQ) is a derivative of chloroquine (CQ) and was produced with the introduction of the hydroxyl group into chloroquine in the year 1946. CQ and HCQ both are structurally similar weak bases, which are derivatives of quinoline. HCQ is an aminoquinoline [46], the presence of hydroxyl group influences the conformational changes and water solubility. In animal trials, it was found that the HCQ was nearly 40% lesser toxic than CQ [47]. HCQ is generally used to prevent or treat uncomplicated malaria in regions where people did not respond to CQ treatment [46]. These medications belong to a class known as disease-modifying antirheumatic drugs (DMARDs). They can reduce skin problems in lupus and prevent swelling/pain in arthritis. Recently, CQ and HCQ are both being investigated for the treatment of SARS-CoV-2 due to their anti-inflammatory and immunomodulatory properties [48].
Mechanism of action of HCQSeveral mechanisms of action are proposed to describe the therapeutic effects of HCQ, but the majority of them are based on in-vitro studies. Notably, the relationship between these mechanisms of action and in-vivo clinical efficacy and safety is yet to be fully explained. HCQ is known to have direct molecular effects on lysosomal activity, autophagy, and signalling pathways. Based on various therapeutic involvements of the immune system, the mechanism of action is probably dependent on the infection condition, inflammatory conditions, and affected tissues or organs.
At molecular level Inhibition of lysosomal activity and autophagyOne of the important modes of action of HCQ is interfering with lysosomal activity and autophagy. It accumulates in lysosomes and inhibit its normal function. In-vitro, CQ can destabilize lysosomal membranes and promote the release of lysosomal enzymes inside cells. The ability of CQ and HCQ to interfere with lysosomal activity has been extensively documented [49]. This mechanism inhibits the function of lymphocytes and have immunomodulatory and/or even anti-inflammatory effects. The anti-inflammatory effects could be a result of impaired antigen presentation via the lysosomal pathway. Lysosomes contain hydrolytic enzymes, in association with other vesicles, perform autophagy by digesting materials from inside the cell (endocytosis) or outside the cell (phagocytosis) (Figure 2). Lysosomes are engaged in recycling cellular substrates, antigen processing, and MHC class II presentation, which indirectly promotes immune activation [50]. Normally the lysosomal pH is maintained optimum to keep its enzyme active. HCQ might impair the maturation of lysosomes and auto-phagosomes by increasing the pH of endosomal compartments and inhibit antigen presentation. In assumption, the available studies suggest that HCQ inhibits immune activation by impairing or inhibiting lysosomal and autophagosome functions (Figure 2). One study has identified palmitoyl-protein thioesterase 1 (PPT1) as a potential lysosomal target that binds and inhibits PPT1 activity [51]. PPT1 is an enzyme involved in the catabolism of lipid-modified proteins. Notably, PPT1 is found to be overexpressed in the synovial tissue of patients with rheumatic arthritis (RA).
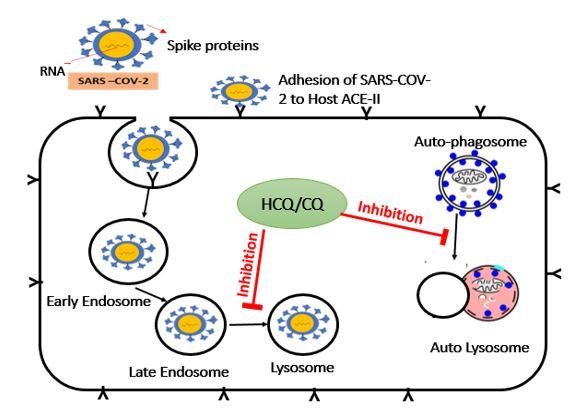
Figure 2: Effect of HCQ/CQ on primary infection process of SARS-CoV-2. HCQ/CQ inhibits the various process of SARS-COV-2 infection cycles such as late-stage endosomes, lysosomes, and autophagy.
Inhibition of signalling pathwaysChanges in endosomal pH can interfere with toll-like receptors, for example, TLR9 and TLR7 processing hence, CQ and HCQ might prevent TLR activation upon extracellular stimuli by changing the local pH. HCQ might block TLR9 signalling at the intracellular level by inhibiting TLR-ligand interactions by directly binding to nucleic acids (Figure 3). This hypothesis is backed by an analysis based on fluorescence spectroscopy and surface plasmon resonance which showed that antimalarial drugs directly inhibit CpG-TLR9 communications [52]. In addition to TLR9 signalling, CQ can also inhibit RNA-mediated activation of TLR7 signalling. Though the exact modes of action for inhibiting TLR7 and TLR9 requires further delineation, the inhibition of TLR processing and binding are likely to be the central mechanisms of action. Another potential mode of action of HCQ is interfering with cyclic GMP- AMP (cGAMP) synthase (cGAS) and the activity of cGAS is repressed by ligand binding. The cGAS-stimulator of IFN genes (STING) pathway is the main cause of the type I IFN response. cGAS inhibitors are at present in advancement for the development of treatment of inflammatory rheumatic diseases [53].
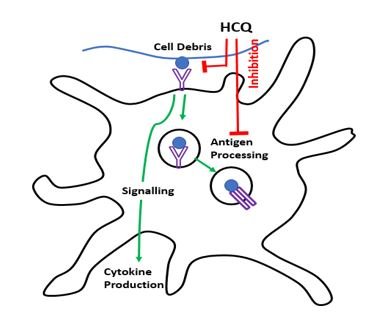
Figure 3: Effect of HCQ/CQ on signalling pathways of Antigen-presenting cell (APC), where HCQ particularly affects the virus by blocking antigen processing and recognition.
At cellular level Cytokine production and immune activationHCQ can inhibit TLR pathways to decrease the formation of cytokines. In in-vitro studies, it was found that HCQ had inhibited the production of IL-1, IL-6, TNF, and IFNγ by mononuclear cells. Furthermore, treatment with HCQ had inhibited the production of TNF, IFNα, IL-6 and CCL4 in pDC and NK cells co-cultures stimulated with RNA-containing immune complexes. In a study, it was found that, IL-1 receptor-associated kinase 4 (IRAK4) had reduced the production of cytokines from peripheral blood mononuclear cells (PBMCs) better than HCQ [54]. The IRAK4 affect the expression of 492 genes, however, HCQ was reported to modify only 65 genes. This study indicated that HCQ has a remarkable inhibitory effect on cytokine production and gene expression, despite its effects on few genes [54]. In another study, it was found that treatment with HCQ, reduced IFNα levels in serum of patients with SLE (Systemic Lupus erythematosus) [54]. The long-term treatment of rheumatic arthritis patients with HCQ at the dosage of 200-400mg/day had reduced the circulating levels of IL-1 and IL-6. The anti-inflammatory effects of HCQ could be attributed in part to the inhibition of immune activation including inhibition of lysosomal activity. Indeed, treatment with HCQ is associated with a dose-dependent downregulation of the co-stimulatory molecule CD154 on CD4+ T cells from patients with SLE. The downregulation is accompanied by a decrease in intracellular Ca2+ mobilization and translocation of nuclear factor of activated T cells cytoplasmic 1 (NFATc1) and NFATc2. However, to be confident on the direct effect of antimalarial drugs on altered cytokine production requires further studies.
Cardiovascular effectsHCQ can able to prevent the development of thrombotic complications in a patient with systemic inflammation and primary Antiphospholipid syndrome (APS). Patients with inflammatory rheumatic diseases are at a higher risk of developing cardiovascular complications when compared with the general population [55]. Treatment with HCQ appears to provide long-term benefits by reducing the risk of cardiovascular events, lowering fasting glucose levels, and reducing hyperlipidaemia. In a study, patients with SLE were treated with combined low-dose aspirin and HCQ as well as aspirin and HCQ, the results were found superior in combination than aspirin or HCQ alone in terms of preventing cardiovascular complications [56]. However, sufficiently large and controlled studies are needed. HCQ can also potentially inhibit antiphospholipid antibody binding by which, it can reduce the pro-coagulatory state in autoinflammatory diseases or platelet aggregation.
Possible role of chloroquine (CQ) and hydroxychloroquine (HCQ) against COVID-19CQ and HCQ were reported to share similar mechanisms of action against COVID-19 [47]. In the earlier outbreak of SARS, HCQ was tested to have in-vitro anti-SARS-CoV activity. But, HCQ becomes a safer option than CQ because of the narrow therapeutic and safety index margin. Yao., et al. (2020), found that HCQ was more potent than CQ in treating SARS-CoV-2-infected Vero cells [57]. It was demonstrated that the safe dosage (6-6.5 mg/kg per day) of HCQ sulfate concentration possibly produces serum levels of 1.4-1.5 μM in humans. To efficiently treat patient with nCOVID-19 infection it is recommended to give 400 mg of HCQ orally per day for 7 to 10 days. It was observed that 70% of HCQ-treated cases were found negative comparing with the control group (12.5%) [58]. It is reported to inhibit SARS-CoV-2 infection in 3 to 6 days. HCQ individually inhibits the SARS-CoV-2 infection whereas; in combination with other drugs, its efficacy was increased. Gautret., et al. (2020), used azithromycin (known to inhibit Zika and Ebola viruses) in combination with HCQ to treat COVID-19 patients [58]. The results were encouraging and on day 6th, 100% of cases were cured hence it is important to understand how HCQ is inhibiting the SARS-CoV-2 infection [58].
HCQ is a weak base known to raise the pH of acidic organelles (endosomes/lysosomes) [49]. Hence, changes in pH are assumed to prevent viral entry, transport, and post-entry stages as well. In addition to this, it is confirmed that HCQ effectively inhibits the entry of SARS-CoV-2 by changing the glycosylation of viral protein. HCQ also inhibits the release of the SARS-CoV-2 genome by blocking the transport of virus from early endosome antigen 1 (EEA1)-positive (EEs) to endosomal-lysosomal protein LAMP1+ (ELs) [59]. It was earlier reported that HCQ has high affinity towards sialic acid and ganglioside, which competitively inhibit the binding of viral S protein to ganglioside. Therefore, HCQ treats the nCOVID-19 patient by changing pH, protein glycosylation, prevent binding of S protein to gangliosides and blocking transport mechanism. In addition to inhibiting viral infection, HCQ has immunomodulatory property and can suppress the immune response [60]. Therefore, it may also attenuate the inflammatory response in nCOVID-19 cases [47]. Cytokines such as IL-6 and IL-10 have been reported to be increased in response to SARS-CoV-2 infection which may lead to cytokine storms followed by multi-organ failure and death [40]. HCQ was reported to influence the production of these interleukins and hence suppresses the hyperactivated immune response.
Global overview on regulatory aspectsThe Food and Drug Administration (FDA) is a federal agency of the United States (US). Under certain conditions such as public health emergency, the FDA may authorize the use of investigational unapproved drugs or therapies. HCQ was an FDA approved anti-inflammatory and antimalarial drug. Whereas, CQ was an approved antimalarial drug. But to date, no medicines or vaccines are approved by the FDA against the COVID-19 disease. However, on March 28th, 2020 the FDA has given an emergency use authorization (EUA) for CQ and HCQ drugs donated to the strategic national stockpile (SNS) to be used for the patients infected with SARS-CoV-2. SNS can distribute these drugs to states and doctors can prescribe and treat adults and adolescent patients who weigh ≥50 kg and have been hospitalized with severe COVID-19 infection. EUA states that fact sheet indicating the information on usage, potential known risks, and drug interaction should be made available to health care providers and patients. Potential patients can get these medicines by two means. First, they may approach pharmacies with an off-label prescription issued from a licensed doctor. Secondly, the patients may also obtain through SNS. Anticipating the increased demand, FDA had published product-specific guidances (PSGs) to support the new generic development of these drugs. The PSGs, for these two drugs mention that these are AA rated (No, bioequivalence problems in conventional dosage forms) and in-vivo studies are not necessary [61]. European medical agency (EMA) is involved in the evaluation of medicinal products of the European Union (EU). EMA states that the patients suffering from COVID-19 can use these drugs under a doctor’s supervision and necessary information about the usage should get from the doctor or pharmacist. EMA also states that the medical professionals can’t prescribe these drugs for more than the required durations and these drugs only should be used in case of chronic disease conditions. The health care professionals can use these drugs only for clinical trials and for outside clinical trials, they should follow the nationally established protocol [62].
Indian Council of Medical Research (ICMR) is accountable for the design, management, and advertising of biomedical research in India. On 23/03/2020, the National Task Force (NTF) constituted by ICMR recommends the use of CQ and HCQ for the treatment of high-risk individuals. The task force recommends only high-risk people can be subjected to chemoprophylaxis with HCQ. The high-risk individuals and dosage recommended by NTF is as follows. The asymptomatic health care workers should take 400 mg of HCQ two times on the first day, followed by once a week for the next seven weeks. The recommended drug must be taken along with the meals. Whereas, the asymptomatic household contacts of laboratory-confirmed cases, should take 400 mg dose two times on day 1, followed by once in a week for another three weeks at 400 mg dose and it should be taken along with meals. The task force restricts the recommendation of prophylaxis in children below 15 years of age and for the person with known cases of retinopathy and having a hypersensitive reaction to HCQ and 4-aminoquinoline compounds. ICMR recommends only the above-mentioned people should take the recommended dose as preventive measures only. However, they should follow all prescribed public health measures such as maintaining safe social distance (minimum 1 meter), respiratory guidelines, frequent hand washing, and also, they should use all kinds of personal protective equipment [63].
The other regulatory bodies such as Brazilian Health Regulatory Agency (Anvisa), Australia’s Therapeutic Good Administration (TGA), Medicines and Healthcare Products Regulatory Agency (MHRA) doesn’t recommend CQ and HCQ for treatment of COVID-19 and warns the public about self-medication due to serious health risks associated with the drug usage. These bodies reinforce necessary clinical trials on representative human samples to prove the safety and efficacy for approval. World Health Organization (WHO) is following all the clinical trials conducted on control of COVID-19 from various research organizations. However, due to the unavailability of efficacy and safety data from clinical trials WHO is not recommending the use of anti-malarial drugs (CQ and HCQ) for the treatment of COVID-19 [64].
It is clear from research data and clinical trials that controlling inflammatory immune responses is as crucial as targeting the virus to stop the progression of the disease. Doctors and researchers have tried several drugs alone or in combinations for helping COVID-19 patients. However, to date, there is no approved drug against this newly emerged disease. Historical studies on SARS and MERS suggests that the hosts’ immune responses (innate and adaptive) against SARS-CoV-2 are similar to these viruses. Therefore, at present, the vaccines and drugs which were used against SARS and MERS are being tested against COVID-19. Amongst all, antimalarial drugs hydroxychloroquine has received enormous attention due to its immunomodulatory property and could be a potential therapy to treat severely affected COVID-19 patients. However, human immune response and the timing of immunomodulation therapy is crucial to get positive outcomes. As an immunosuppressant, HCQ may potentially affect the antiviral immune response, therefore, clinicians should decide the timings to use such medications based on patients’ age, medical condition, and severity of the infection. Moreover, the early intrusion of such therapy in infection-associated-hyper inflammation is considered as a strategic aspect to get recovery against COVID-19. As HCQ is a broad-spectrum antiparasitic, anti-rheumatic, immunity booster, immunomodulatory and immunosuppressant, several countries have included this therapy for COVID-19 treatment, irrespective of the unavailability of enough clinical and scientific data to support the use of HCQ against COVID-19. In India, the usage of HCQ drug is recently approved by ICMR to combat against COVID-19 infection as well as to utilize this drug as a prophylactic measure for frontline health workers. However, with current ambiguity regarding the usage of HCQ drugs to treat COVID-19 patients, it is important to understand the potential risks and benefits of this drug. Ongoing clinical trials will provide significant data for an enhanced understanding of the potential role of HCQ in the treatment and prevention of COVID-19. Also, additional studies on host immune responses against SARS-CoV-2 are equally crucial to understand the dysfunctional outcome of immune responses, such as cytokine storm and hyper-inflammation in severely affected COVID-19 patients. Understanding of correlation between immune responses and disease severity may also prove to be a game-changer strategy to finalize the antiviral drugs and adjuvants to control COVID-19.
The authors declared that there is no conflict of interest exist in the publication.
Copyright: © 2021 Sunita Singh., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff