Coulic Véry1*, Novikov VN1,3, Mboti F1,4 and Delrée P2
2Translational Medicine Laboratory of the Brussels Free University, Brussels, Belgium
3NV Sklifosovski Research Institute of Emergency Medicine, Moscow, Russia
4CHU Brugmann, Department of Thoracic, Endoscopic and Abdominal Surgery, Brussels, Belgium
*Corresponding Author: Coulic Véry, Translational Medicine Laboratory of the Brussels Free University, Brussels, Belgium.
Received: May 29, 2021; Published: 00-00
Citation: Coulic Véry., et al. “Foetal Organ Implantation into Adult Animals: A Model for In Vivo Culture of stem cells?". Acta Scientific Gastrointestinal Disorders 4.7 (2021): 80-93.
Background: Presently stem cell implantations are more and more developed and applied in clinics as alternative and complementary solutions to adult organ transplantation because of the growing demand and capacities to provide these interventions, while lack of donors is patent. But some limitations of stem cell use remain (for instance integration within the recipient organism of engineered tissues and organoids obtained in vitro from stem cells). The use of foetal organ implantation into adult animals may be an alternative for in vivo study of stem cell development and evaluation of the host participation to this process. The objectives of this work were o try different foetal organ implantations into adult animals (part I) and to evaluate their use for repairing experimental lesions of some adult organs (part II).
Material and Methods:
Result:
Conclusion: Implantation of different foetal organs into syngeneic adults may constitute a valuable model for theoretical studies of in vivo stem cell differentiation and organoid growth. The ear implantation site deserves special attention. Some interesting applications are possible and worthwhile to be discussed and developed.
Keywords: Foetal Organ Development; Precursor Cells; Stem Cells; Regenerative Medicine; Reparative Surgery; Surgical Experimental Models; Heart Repair; Oesophagus Defect Reconstruction; Diabetes Treatment
BW: Body Weight; DM: Diabetes Mellitus; ESC: Embryonic Stem Cell; FH: Foetal Heart; FI: Foetal Intestine; FL: Foetal Liver; FPa: Foetal Pancreas; FOE: Foetal Oesophagus: FOI: Foetal Organ Implantation; IGF-1: Insulin-Like Growth Factor; M: Mean Value; MRI: Magnetic Resonance Investigation; MSC: Mesenchymal Stem Cell; PDDM: Protein Deficit Diabetes Mellitus; PTH: Parathyroid Hormone; PTHrP: Parathyroid Hormone Receptor Protein; RNA: Ribonucleic Acid; SD: Standard Deviation; US: Ultra Sound
Taking into account the problems of adult organ transplantation (graft procurement, life lasting post transplantation treatment and its complications [1-7]), other solutions are presently envisaged in reparative/regeneration medicine and surgery: use of stem cell obtained from embryonic origin (ESC) or derived from different adult tissues by dedifferentiation in vitro (MSC) [8-10]. Studies about stem cell observation and use are developing in three directions: 1) comprehension of embryogenetic growth pattern [11-15], 2) investigation of the pathogenesis of some diseases and hence of possibility of influencing their course [16-18] and 3) practical use for tissue and organ repair [8,10,19]. Human organoids produced in vitro are more and more used for developmental, physiology and pathology investigations, for therapeutics trials, but not really in reconstructive surgery yet [20-26]. Presently, stem cell creation has now extended to industrial production for clinical applications [8,9,27-29]. But some questions remained open such as the degree of integration of implanted stem cells, their real role in restoration of leased organ function (replacement or boosting the own organ resources). In fact, stem cell use has fair results in tissue repair such as bone, cartilage and tooth structures, and haematopoietic and liver tissues. Biology of the ectopic development of the grafted tissues and growing organoids still remains weakly investigated, especially the possibilities of innervation by the host or inclusion into the neuro-humoral system of the organism regulation [30]. And in any way, stem cell and organoid are the result of an artificial production in vitro that may explain their difficulties really to become integrated into the organism where they are implanted even when this implantation is autologous.
The question is a little different, when we consider foetal tissue and organ transplantation.
Foetal organ transplantation into adult organisms is an old problem which study began in the 50-ies of the XX century with foetal heart grafting [31,32] and extended later to foetal digestive organs [33,34].
Foetal organ transplantation has two faces: theoretical one - how perfect is the ectopic foetal organ growth, and practical one - how suitable the foetal organ graft is for reparative surgery. The main foetus organs were investigated: heart [35-46], digestive tract (intestine [47-51] oesophagus and stomach [52-57])], pancreas [58-65]; different digestive organs together [66-71], liver [72-78], lung [79], kidney [80], some of them more than others. The first studies on the foetal heart and intestine implantation into different sites (subcutaneous, in occulo, under spleen capsule and others) have already shown that the foetal implants could give growth to “adult-like” formations able, in certain conditions, to manifest functional activity. For instance, the foetal intestine, after sub cutaneous implantation on a rat spine was able to secrete if a stoma was managed [51], a foetal heart implanted into the anterior chamber of the eye was able to beat and react to adrenalin and acetylcholine injected to the host [35].
Implants of foetal pancreas were shown to be able to influence the manifestations of diabetes mellitus [60,61,66].
But the moratorium imposed from 1970 up to 2009 to the studies involving embryos and foetuses has prevented the development of all side investigations [79]. And the possibilities of the “natural” in vivo growth process of ectopic cell, tissues and organ were poorly explored.
The aims of the present work was to try organ in vivo cultures by means of foetal organ implantations into adult animals (part I) and to evaluate their possibilities of use for repairing experimental lesions of adult organs (part II).
Experiments were carried on more than 650 adult Wistar and Fischer rats, and C57Bl and BALBc mice both sexes, aged 2 - 6 months, according to Bioethics rules, and allowed by local Ethics Committee protocols NN°50, 508 and 690. All the surgical interventions and/or manipulations were performed under anaesthesia or sedation of the animals. The study was provided during a period beginning in 1978 [36] and extending up to 2020. The complete enumeration of the experimental series is presented in table 1.
|
Series (implants) |
Implantation site |
Animal nb (recipients) |
Observation delay |
|
Fetal esophagus |
Ear, Neck |
10 30 |
6 months 9 months |
|
Fetal stomach, intestine |
Ear Neck |
> 100 23 |
12 months 6 months |
|
Foetal umbilical cord |
Ear |
20 |
4 months |
|
Foetal heart (FHI) |
Ear Thorax |
30 40 |
14 months 12 months |
|
Foetal liver (FLI) |
Ear Spleen hile |
29 21 |
12 months |
|
Foetal pancreas (FPI) |
Ear Spleen hile |
104 14 |
9 months |
|
Oesophagus lesion + (GFOI) |
Neck |
20 + 5 |
13 months |
|
Heart lesion Heart lesion + FHI |
Thorax |
20 40 |
6 months |
|
DM (SD or PDD) DM + FPI |
Ear, abdomen |
20 + 37 34 + 38 |
6 months |
Table 1: Number of animals and experimental series.
GFOI: Grown Foetal Oesophagus Implant; SD: Diabetes Induced by Streptozotocin; PDD: Protein Deprivation Induced Diabetes.
These experiments were performed in syngeneic system of transplantation to avoid bias from immunologic rejection reaction.
The schema of different operations is presented on figure 1.
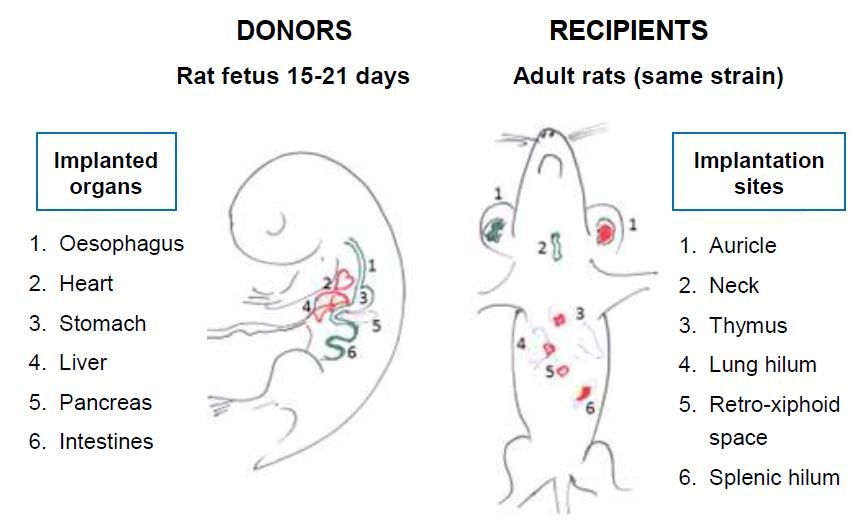
Figure 1
Donors were foetuses aged 14 - 20 days in utero. Under Fluorotane/Isofurane 4% pre-anaesthesia, and after intra peritoneal injection of Nembutal© 0.75 mg/kg and of Temgesic© 0.5% 0.2 ml as main anaesthesia, laparotomy of the gravid female was provided and the foetuses were extracted, the target organ was isolated and placed in a cup with saline at ambient temperature. In 10 cases donors were animals having received a foetal intestine segment which have begun to develop. A part of this growing implant was used as new graft (pricking or subculture).
Recipients were anaesthetized in the same way (except that last years, Nembutal was no more used and replaced by a mixture of Ketalar®, Diazepam 1% and Temgesic® 1% in equal quantities of 0.1 ml/100g BW), after what a subcutaneous pouch was created within 2 - 3 mm after skin cut and blunt separation from the subcutaneous layer of the ear pavilion. A piece of oesophagus, stomach, intestine, liver, pancreas (volume 2 - 4 mm3) or the whole heart was introduced into the subcutaneous pouch. The skin wound was closed either by 8°° Ethilon® stich or by clay (Nobecutane©). The same principle was used for implantation at the anterior neck region; the piece of foetal organ being placed at the caudal top of the salivary gland.
When thorax site was used, after complementary subcutaneous injection of Atropine 1% 0.2 ml, intubation and start of artificial ventilation (UNO - Intermed - Penton, Sigma Delta, Netherland), a classical sternotomy was performed. The implant was either dropped into the cavity, or introduced under the pleura of the lung hilum, or under the thymus capsule, or fixed on the heart apex. After what the thorax was sutured by stiches layer after layer: sternum (Vicryl 2°°), muscles and skin (Vicryl 4°°).
In the case of abdominal implantation, laparotomy was performed and the implant was either dropped into the cavity or placed under the visceral peritoneum in the region of caecum or spleen hilum. The abdominal wall was sutured in 2 layers: peritoneum and muscles by a continuous catgut or Vicryl 4°°, the skin - by Vicryl 4°° stiches.
Some experimental models of organ lesions were also used to test the foetal organ implantation as a way to correct them. They included diabetes mellitus induced by Streptozotocin® intra peritoneal injection (75 mg/kg) or by protein deprivation, and also oval or circular resection of the cervical oesophagus and thermic lesion of the heart apex, which are described other where [46,57].
After surgery the animals were placed into individual cages during the whole observation period in order to avoid competitive situations able to influence the survival and general condition of the animals.
Pilot study of human foetal pancreas implantation was also provided in 60 diabetic patients (1980 - 1992, Moscow, Academy of Medicine Scientific Research Institute of Artificial organs and Transplantation and District University Clinic n°64; authorization by the USSR Ministry of Health). After enlightened consent of the patient and the responsible gynaecologist, still born foetuses BW < 500g were used as donors. Pancreas was procured and immediately transplanted into a subcutaneous pouch of the para umbilical region of the recipient under local (Xylocain 0.5%) anaesthesia [60].
The investigation methods included:
The observation delays ran from day 0 to day 600. Euthanasia was provided by intra peritoneal injection of pentobarbital 2*, 1 ml/100g BW.
The follow up of human recipients was usual for diabetic patients after any surgery including frequent blood glucose determination and assessment of the implant condition by regular US exploration of the anterior abdominal wall.
Experiments have shown that some conditions are required to ensure the success of the implantation:
|
Ischaemia (min) |
2 weeks |
4 weeks |
|
< 20 min 30 - 50 min 50 - 60 min = or > 60 min |
31/31 = 100% 53/53 = 100% 15/16 = 94% 3/5 = 60% |
29/29 = 100% 44/47 = 91% 8/12 = 66% 2/4 = 50% |
|
Total implants |
102/108 |
83/92 |
Table 2: Survival of the syngeneic foetal heart implant (survival number/total implants) depending on “ischemia” delay.
NB: In all the animals both ears were used.
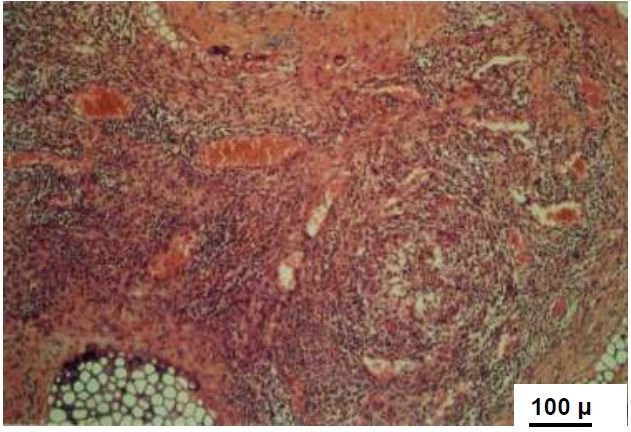
Figure 2
Implantation under thymus, salivary gland capsule as well as under the spleen hilum or the ileocecal angle visceral peritoneum, was successful in 50 - 75% of the cases.
Implantation into an ear pavilion subcutaneous pouch presented the possibilities of visualization of the implant evolution, of the measure of the graft dimensions and vascularization features (Figure 3), as well as biopsies procurement.
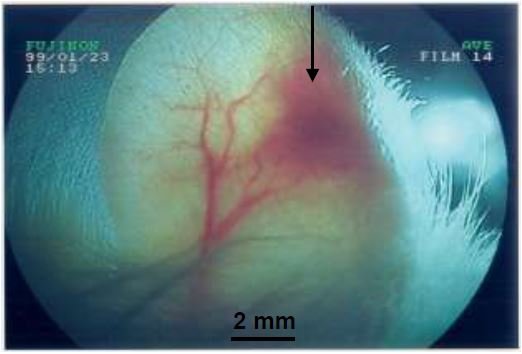
Figure 3
During the first days, independently on the implanted foetal organ concerned, the evolution of the implant was the same - the specific organ structure was replaced by a kind of infarcts with cell apoptosis and necrosis and the predominance of undifferentiated cells (Figure 4).
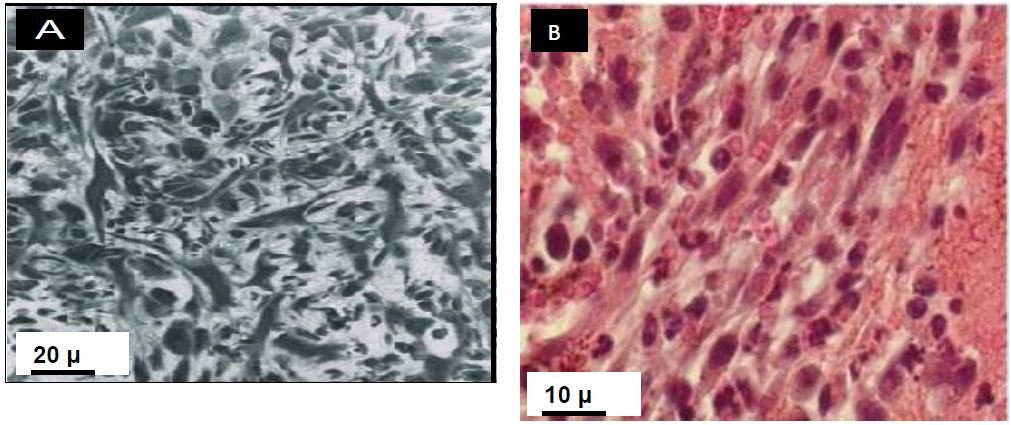

Figure 4
At these observation delays it was even difficult to identify the nature of the implant.
Penetration of recipient capillaries into the graft and their connection with the graft lacunas were observed about 5 - 7 days after operation.
During the next weeks, differentiation of tissues was realized according to ontogenetic pattern specific to the implanted organ (Figure 5).
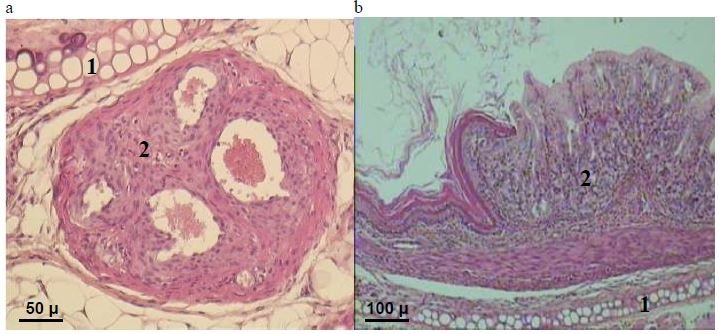
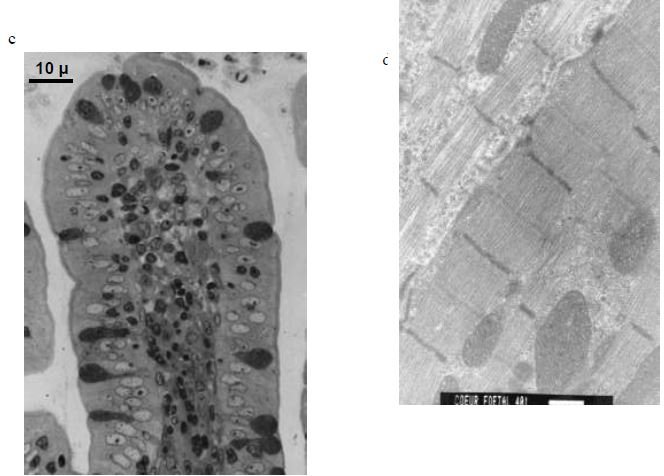
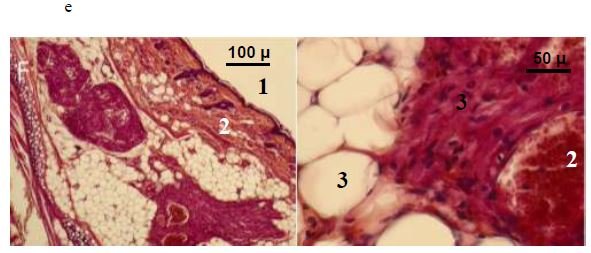
Figure 5
An exception was noted when umbilical cord was implanted: the placental end did not develop as an organ, and the foetal third containing allantois, developed as a small intestine.
As an exception, teratomas were observed in 3 cases, when very young donors (BW < 1g) were used [See also 90, 91]. If the whole material (parts 1 and 2) is considered, that is more than 650 operations. 6 cases were detected, i.e. 0.36%.
According to first investigations IGF-1, PTH and PTHrP levels were slightly elevated at day 7 - 14 post operation. PTH was high in normal foetal intestines and slowly decreased after birth. In the case of ectopic development a slight decrease was noted during the first days, that corresponded to the necrosis and apoptosis noted in the graft. At days 7 - 9 a pike of activity was expressed, corresponding to the beginning of the re-formation of the grafted intestine. On the contrary, PTHrP expression has shown a trend to decrease. As to IGF-1, the elevation of its blood level was maximal reaching 150 - 200% of its initial and control levels at the end of the second post operation week and remained significantly higher than control during the further 4 - 6 months (Table 3).
|
Observation delay |
Foetal intestine |
Foetal heart |
Foetal pancreas |
Significance (vs control) |
|
Control (intact) |
460 ± 31 |
460 ± 31 |
460 ± 31 |
|
|
Day 4 |
599 ± 130 |
589 ± 37* |
689 ± 200 |
*p < 0.01 |
|
Day 9 - 14 |
1120 ± 200* |
nm |
713 ± 58* |
*p < 0.01 |
|
Month 2 - 3 |
922 ± 85* |
nm |
672 ± 25* |
*p < 0.01 |
|
Month 6 |
624 ± 56* |
608 ± 80* |
498 ± 11 |
*p < 0.01 |
Table 3: First results of IGF-1 determination in recipient sera (ng/ml).
The grown implants of foetal heart, intestine, stomach, and oesophagus have proved to be functional: motility, secretion for intestine and stomach, presence of a cardiac rhythm and blood flow for the heart were detected (Figure 5 and 6). As to liver and pancreas, adult structures were obtained but not an organ functioning as a whole. So liver has shown bile system and hepatocyte columns with sinusoids, but no sign of bile elaboration. The grown foetal pancreas developed pancreatic tubes, sometimes acinar formations and endocrine cells immune-positive for insulin, glucagon and somatostatin. But no pancreatic organization was observed. Nevertheless foetal pancreatic implants have shown functional activity (See also [49,51,57]).
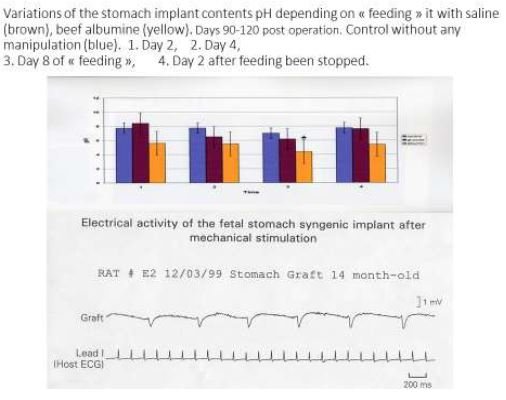
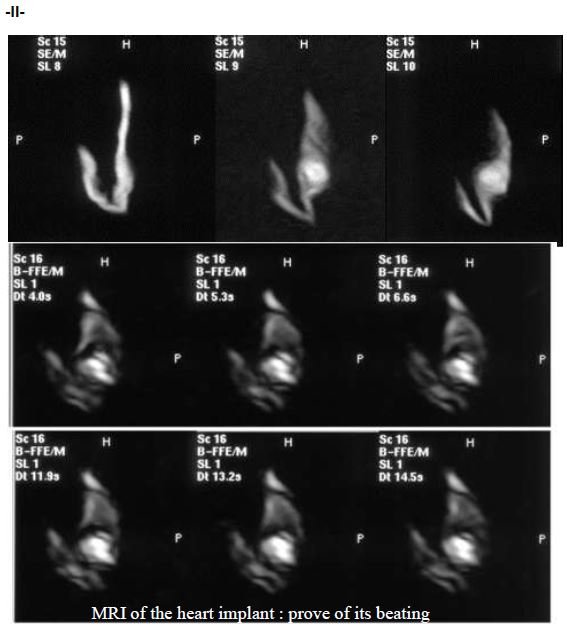
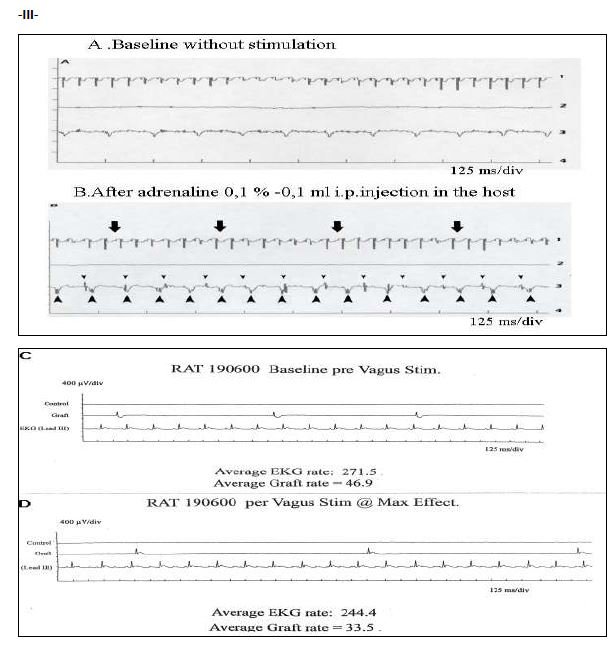
Figure 6
In late delays (8 - 11 months) the implants have shown signs of aging: fibrosis or adipose degeneration (See figure 5e).
In the short series with “pricked” or sub cultured growing foetal intestine implant into another adult rat at the ear site, at days 14 intestinal mucosa with villi formation was observed in the secondary developing implant (Figure 7).


Figure 7
Part IIExperiment results have been presented in several publications [60-64].
They can be summarized as following:
As shown in our and different authors experience, analysis of foetal organ implantation results are conditioned by different external and internal factors influencing the graft development. Among them “ischaemia” duration, implantation site peculiarities, especially vascularization, general condition of the recipient, but also the foetal organ peculiarities are to be considered.
The comparison of the different surgical models of foetal organ implantation used in our study has shown that the best results (up to 95 - 100% success) were obtained in the case when the warm ischemia duration did not excess 50 min, and the shortest was the best. We did not use cooling of the procured organs, as far as preliminary tests were negative: cold altered foetal cell condition.
Important too that the implantation site was well vascularized: under the skin, gland capsules or visceral peritoneum, or within a subcutaneous pouch of the ear pavilion. Spleen or liver or kidney superficial parenchyma are well known implantation sites; which also satisfy to the same criteria of rich vascularization, as well as anterior eye chamber [35,36] and probably the vestibule cochlear nerve [80].
The subcutaneous pouch of ear pavilion, first proposed by Fulmer., et al. in 1963 [32], seems to be an original implantation site and has shown different advantages: simple, easy to perform and not very traumatic operation, well tolerated by animals, allowing visual observation, measures, biochemical and physiological investigations of the implant, procurement of biopsy material. Last preliminary experiments suggest that it might be used for precursor cells culture and selective development. The only inconvenient seems to be the limited extension volume for the implant growth.
The neck implantation site ensured place enough from even enormous growth of intestine or stomach adult-like cysts. In our experiments we did not ensure the exit of secreted mass, though it is possible and has spontaneously occurred in some cases. This model might present interesting perspectives for physiological studies of the grown implant (For instance pH determination, motility detection and so on).
The evolution of the implanted foetal organ has shown different phases. First, a “destructuration-dedifferentiation” phase during the first week after operation. From day 2 to day 5 - 7 the observed picture may be interpreted either as regression, dedifferentiation of the organ structures, or as the result of mature cells necrosis whereas weakly differentiated ones survived and gave a new development after a while. Unfortunately, up to now we have not had the possibility to perform the necessary tests with stem cell marking or determination of host/graft cells into the mixture of lymphocytes, fibroblasts and other not identified cells. Interesting that at this moment it was difficult to identify the very origin of the graft (See figure 4A and 4B). Phase 2 is characterized by vascularization of the graft and differentiation of the “magma” cells which formed an adult like organ at the end of the first post implantation month. During phase 3 the structure stabilized and function developed, maintaining during several months. Phase 4 was characterized by aging phenomena, morphological and functional degradation.
Nevertheless, during the second phase of re-differentiation, the reconstitution and development of the implanted organ was specific and never deviated from the ontogenetic pattern. Even when we tried umbilical cord implantation and obtained the growth of an intestine, that may be explained by the presence of the allantois, coming from endoderm and primary intestinal tube. These observations mean that re-differentiation probably occurs from precursor cells already organ determined. This also signifies that the first phase is worthwhile further investigations not only for cell identification, but also in order to influence both their differentiation and development, and possibly to modulate their antigenicity.
It is necessary to note that we observed the growth of teratoma in 6 cases (out of more than 650 operations), including 2 cases of malignancy. This was previously discussed [81,82], but it is important to underline that it always occurred: 1/when the donor was very young (< 1g BW, < 12 day in utero age) and so could contain embryonic multipotent stem cells, and 2/ when the foetal organ was implanted into a zone of the adult organism, where stem cells could be easily mobilized (posterior mediastinum, cervical oesophagus zone). The absence or the small quantity of pluripotent stem cells in the implant procured from donors in the last third of gravidity, might be a warrant of its correct development, without tumour deviance.
We have also observed that only hollow organs containing an intramural nervous system or a conduction system and expressing motility capacity as oesophagus, stomach, intestines and heart, were reconstituted as whole organs with organized and long lasting effective physiological activity. As to liver and pancreas, their constitutive elements were present, but coordinated activity of the organ as a whole was absent (for instance, no sign of exocrine secretion both in pancreas and liver was detected). Nevertheless, functional activity was patent: in pancreas - ability to influence diabetes evolution in rats after Streptozotocin injection [60,62,63], in liver - capacity to correct specific pathology [73,76]. These organs are innervated differently, without a “peripheral brain” within them. Is this the cause of the different evolution of the implant? Besides, studies about re innervation of stem cell or islet cell implants were started but without strong conclusions].
Interesting also to observe that some growth factors values have been elevated in the graft tissue homogenate and in the recipient blood after operation. Both PTH/PTHrP expression and significant growth of IGF1 in the recipient serum were registered beginning from the second week after operation (beginning of the 2d phase of the graft evolution) when the first connexions between the host vascular web and the graft are realized and the graft began to differentiate again. Later the PTH and PTHrP level evolution did not significantly differ from control. On the contrary the IGF1 increase reached up to 150 % and more than its initial value. This elevation lasted all through the second and third phases, during which the implant morphologically and functionally looked like an adult organ. Interesting that boosting IGF-1 delivery by the liver has also enhanced the success rate of foetal pancreas implantation [62,65,71].
Following the previous observations and reflexions, the question of the respective role and mutual interactions of donor and recipient in the implant development must arise. For instance, why did the host IGF1 levels remain significantly high during months that corresponds to the 2d and 3d phases of the foetal intestine and heart implant growth? They normalized later at the 4th phase when aging and fibrous or adipose degeneration of the graft developed. What is the origin of this phenomenon and its mechanisms? Where the IGF1 comes from: from the graft, from the host liver, from both? Is the IGF-1 increase a promoting factor of the implant development or a consequence of the implantation and development of the graft, or both? What are the adult organism limits of stem cell mobilization for tissue and organ repair? and interaction with the graft? How to influence these phenomena and avoid deviances like tumour formation? Nervous plexus and neurons were described in the digestive tract foetal implants: what is their origin - the graft stem cells or a penetration into the graft of host nervous system?
Presently this work cannot give any answer neither to the above mentioned questions nor to the question of the origin of the grown implant cells (only implant or with host participation). Deeper analysis and complementary investigations are needed. The possibility of the developed implant integration to the host organism needs convincing proofs (that is especially important for heart repair). Implants of digestive organs were morphologically distinct from recipient tissues except when implantation was performed into a lesion site like oesophagus defect. Foetal heart implants behaved in the same manner: when performed in the site of heart apex injury, in last delays close contact with recipient tissues was often observed. But we have no liable proofs of any degree of the implant integration. For that, a liable marking of either donor cells or recipient ones is necessary. It ought to be the aim of further studies. Nevertheless, the results observed in our trials with foetal oesophagus-stomach-intestine use for oesophagus defect repair or with implantation of foetal heart on the site of a thermic injury of the heart apex, were positive. Even foetal pancreas implantation, ensuring endocrine development and function, has given positive results in experiment as in cautious clinical trial. Besides the delay of the graft function was long enough to suppose that islet cells could be renewed, thanks to the presence in the implant of pancreatic tubules, source of endocrine cells of the organ all its life long.
Indeed, the described operations may be proposals of surgical models, simple for execution, relatively cheap and easy in management. They are not exclusive: a lot of foetal organs was not tested here, such as brain, kidney, lung, and other implantation sites are also possible, many of them having been mentioned in literature. Our studies have many common features with organoid creation studies, except that the last are started in vitro and their growth can be obtained from other organs of the same embryonic sheet (for instance intestine crypt cells can give growth to pancreas) by experimental monitoring means [14].
Foetal organ implantations seem to be valuable surgical models, allowing the study of different stem cell category involvement during foetal organ implant growth. They open wide possibilities to experiment in vivo new methods of influencing (boosting, slowing or modifying) the foetal organ graft development. They might be an intermediary step between in vitro studies and clinical applications (for instance, in the field of tolerance research, for instance by donor pre-treatment [58,59]. Are they concurrent with organoid investigations taking into account the tremendous development of research in this domain [9,10,30]? Probably not, they would be rather complementary, because foetal organ transplantation has the advantages to ensure a whole process in vivo with a good vascularization, and a natural humoral environment. So, we hope that this work will be useful for further researches and experimentations in the field of reparative surgery and regenerative medicine.
In summary: FOI presents significant positive sides, such as
Nevertheless FOI significant negative sides are also o be considered, such as:
The authors express their deep and grateful thanks:
None.
Copyright: © Coulic Véry., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff