Mohamed A Mohamed1*, Beri Massa-Buck2, Fern McCree3 and Hany Aly1
1Department of Neonatology, Cleveland Clinic Children’s, Cleveland, OH, USA
2Department of Neonatology, Children’s National Medical Center, USA
3Department of Epidemiology, The George Washington University, USA
*Corresponding Author: Mohamed A Mohamed, Vice Chair, Department of Neonatology, Cleveland Clinic Children’s, Clevland, OH, USA.
Received: April 07, 2021; Published: May 17, 2021
Citation: Mohamed A Mohamed., et al. “Decreased Risk of Intraventricular Hemorrhage in Twin Preterm Gestations”. Acta Scientific Clinical Case Reports 2.6 (2021): 03-09.
Background: The adverse health outcomes of intraventricular hemorrhage (IVH) and severe IVH occurrence in preterm infants are thoroughly documented in existing literature. However, few studies documented the difference in the risk of IVH between singleton and twin gestations. The objective of this study is to examine the association of twin gestation and IVH in very low birth weight (VLBW) infants in a mega data from the United States.
Study Design: A retrospective cohort analysis was conducted on 128,006 preterm infants less than 1,500g at birth, using the Healthcare Cost and Utilization Project - Kid’s Inpatient Database (HCUP-KID) from 1997 to 2012. Prevalence of IVH and severe IVH was compared between two groups: twin versus singleton VLBW infants using chi square and fisher exact test. The analysis was repeated using logistic regression models to control for demographic and clinical confounders.
Results: Of the 128,006 infants, 14.7% were diagnosed with IVH. Singletons were 14% more likely to have IVH than twins (p = 0.001). Multiple logistic regression revealed a significant association between IVH and respiratory distress syndrome (OR: 2.38, 95%CI: 2.16 - 2.63), pulmonary hemorrhage (OR: 3.06, 95%CI: 2.64 - 3.56), patent ductus arteriosus (OR: 1.85, 95%CI: 1.71 - 2.00), pneumothorax (OR: 1.48, 95%CI: 1.22 - 1.80), anemia (OR: 1.39, 95%CI: 1.28 - 1.52) and renal failure (OR: 2.08 95%CI: 1.72 - 2.50). Infants who were female, delivered via C-Section, had history of maternal hypertension, or breech presentation had a reduced risk of IVH.
Conclusion: Twin births were less likely to result in IVH than singleton births. Improved obstetric, perinatal and neonatal care may have resulted in reduced rates of IVH and decreased risk among twins.
Keywords: Intraventricular Hemorrhage; IVH; Twin Gestation; Premature Infants; Very Low Birth Weight Infants
Intraventricular hemorrhage (IVH) of the newborn is rarely present at birth but occurs most often in the first 72 hours of life. This condition predominantly affects premature infants less than 32 weeks gestational age and the risk of IVH is inversely proportional to an infant’s gestational age (GA) or birth weight (BW). In addition to prematurity and gestational age, other factors are associated with greater risks for IVH. Severe asphyxia, respiratory distress syndrome, persistent pulmonary hypertension, neonatal sepsis, pulmonary hemorrhage, pneumothorax have all been shown to increase the risk of IVH [1]. Also, male newborns with very low birth weight are at greater risk of developing IVH than females [1,2].
About 12,000 premature infants are diagnosed with IVH every year in the United States [3]. Although the incidence of IVH among extremely premature babies has decreased from about 50% in the 1980’s to about 15% in recent years, IVH and severe IVH remains one of the leading causes of mortality and morbidities among premature infants [4]. It can lead to various neurological complications such as seizures, cerebral palsy and learning disabilities [1].
It is important to investigate the occurrence and predisposition of IVH and severe IVH among twin pregnancies because twin births present an increased risk for many complications when compared to singleton births. Due to an exaggerated physiologic response in a multi-pregnancy such as a larger uterus, increased amniotic fluid and blood flow, and surge in cardiac output and heart rate; the risk of prematurity for twins increases. Over the past three decades, the rate of preterm birth among twin pregnancies has risen from 48% to 60% [5]. The majority of multiple pregnancies are preterm [6], which increases the risk of many health problems such as low birth weight, respiratory distress and sepsis. Other common complications associated with multiple births are preeclampsia, gestational diabetes, placental abruption, fetal loss and caesarean delivery [1].
Examining IVH risk among twin births would be beneficial to clinicians and mothers when assessing reproductive options. Assisted reproductive technology (ART) such as in vitro fertilization (IVF) has contributed to a 67% increase in twin births since 1980 [7]. ART accounts for 1.5% of all births and 19% of twin births in the US. Out of all ART conceived infants in the US, 43.3% are twin births [7]. IVF twin pregnancies are at greater risk for adverse neonatal outcomes in comparison with naturally conceived twin gestations [7]. The incidence of IVH has been proven to be significantly higher in IVF twin pregnancies [7,8]. Hopeful parents considering fertility treatment may add IVH as a factor in deciding whether to have twins if it is proven that IVH risk is increased with twin birth.
This study examines a mega data from the US that includes millions of newborn infants to assess the relationship of twin pregnancy and delivery with the occurrence of IVH and severe IVH and potentially identify preventable risk factors for IVH among twins.
This is a retrospective cohort analysis that was conducted on 128,006 very low birth weight (VLBW) infants less than 15900 grams at birth who were either admitted via the emergency room or directly to the birthing hospital birth.
Data sourceData was extracted from the Kids’ Inpatient Database (KID), a de-identified dataset produced by the Healthcare Cost and Utilization Project (HCUP), which is sponsored by the Agency for Healthcare Research and Quality (AHRQ). The KID is the largest publicly available all-payer pediatric inpatient care database in the United States containing data from approximately 4 million inpatient stays each year [9]. Ten percent of uncomplicated in-hospital births and 80 percent of complicated births and other pediatric cases were sampled from each frame hospital. This database yields national estimates of hospital inpatient stays for pediatric patients. The information comes from discharge summaries and each hospital stay includes more than 100 data elements both demographic and clinical items. Data elements include discharge status, length of stay, primary and secondary diagnoses and procedures, severity and comorbidity measures, patient demographics, hospital characteristics, payment source and charges. KID has been available every three years since it started in 1997 and the number of states represented has increased from 22 to 44 over time. We included data from 1997 to 2009 for this study.
VariablesAll of the variables used were categorical as present or not present and were defined based on HCUP definitions or International Classification of Disease - Ninth Version (ICD-9) diagnostic codes. The dependent variable was intraventricular hemorrhage (IVH) identified by ICD-9 codes 77210, 77211, 77212, 77213 and 77214. The principal independent variable was type of gestation as twin vs. singleton. Other demographic and clinical independent variables were included in the analyses. Demographic variables were race and sex of the infant. Clinical variables included gestational age (ICD codes 76521 to 76529), birth weight (codes 76501 to 76505), IVH grade (77211, 77212, 77213, and 77214), respiratory distress syndrome (RDS) (code 769), severe asphyxia (code 768), pulmonary hemorrhage (code 7703), patent ductus arteriosus (PDA) (code 7470), apnea of prematurity (code 77082), pneumothorax (code 7702) and anemia of prematurity (code 7766) [3]. Childbirth complications presenting at birth included cesarean section, breech presentation (code 7630) and maternal hypertension (code 7600) [10].
Inclusion/exclusion criteriaPremature infants born with very low birth weight (< 1500g) were included in the study. Infants were excluded if transferred to another hospital because their IVH diagnosis would be unknown. Infants were also excluded if they were diagnosed with any chromosomal defects, had congenital anomalies or renal dysplasia, as these conditions may contribute directly to the occurrence of IVH (Figure 1).
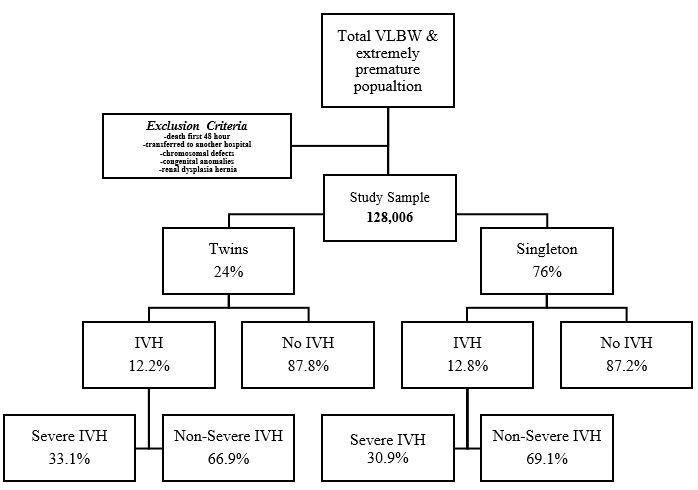
Figure 1: Algorithm.
Statistical analysis methodsStatistical analyses were performed using SAS version 9.3 (Cary, NC). In order to obtain descriptive statistics of the study population, univariable analyses were performed. Pearson’s Chi-square test was used to examine the association between twin gestation and each predictor to determine if there were any differences between groups. Bivariable analyses were performed to examine the association between twin birth and each predictor independently against IVH. Multivariable logistic regression was performed to assess the relationship between all predictor variables on IVH. Differences were compared using unadjusted and adjusted odds ratios, 95% confidence intervals, and p-values. A logistic generalized linear model (GLM) with binomial distribution was utilized for multivariable logistic regression models. The generalized estimating equation (GEE) was used to adjust for clustering by hospital. An exchangeable correlation structure was used. A discharge weight variable was applied to each patient in the dataset in order to produce national estimates. The cluster variable was the HCUP hospital identifier, which was used to account for intra-hospital correlations. HCUP is a national, de-identified dataset available for public use upon submission of a data use agreement. Data Use Agreement forms were completed and submitted to the Agency for Healthcare Research and Quality in order to use the HCUP database. This study was approved by The George Washington University Institutional Review Board (IRB# GWU-020821).
This study included 128,006 infants. Of all the infants included in the study, 76% were singleton births versus 24% twin births. The incidence rate of IVH was 14.7%. Infants were more likely to have a birth weight between 1250 and 1499 grams (36.8% in twins and 27.6% in singletons). Among twins, 44% were white and 16% were black. Singleton births were 31% white and 23% black. Forty-nine percent of twins were males versus 52% of singleton infants. Twins had more cesarean sections deliveries (75.8%) than singleton babies (55.4%). The occurrence of IVH was slightly higher among singleton births (12.8%) versus 12.2% in twins. However, among infants with IVH, grades 3 and 4 (severe) were more prevalent in twins (33.1%) than singletons (30.9%). Complications that were more prevalent in twins were respiratory distress syndrome, pulmonary hemorrhage, patent ductus arteriosus, apnea, anemia, breech presentation and renal failure. Severe asphyxia and maternal hypertension were more likely to occur in singleton births (Table 1).
|
|
Twin 30,857 (24.1) N (%) |
Singleton 97,149 (75.9) N (%) |
P value |
|
Race |
|
|
|
|
White |
13,588 (44) |
29895 (31) |
< 0.001 |
|
Black |
4,978 (16) |
22750 (23) |
|
|
Hispanic |
3.349 (11) |
15504 (16) |
|
|
Asian |
840 (2.7) |
2503 (2.6) |
|
|
Native American |
123 (0.4) |
560 (0.6) |
|
|
Other |
1252 (4.0) |
4295 (4.4) |
|
|
Male Sex |
50,053 (51.6) |
47,003 (48.4) |
< 0.001 |
|
Gestational Age (weeks) |
|
|
|
|
< 24 |
1,906 (9.75) |
8,457 (14.85) |
< 0.001 |
|
24 |
909 (4.65) |
3,690 (6.48) |
|
|
25 - 26 |
2,164 (11.07) |
8,346 (14.66) |
|
|
27 - 28 |
3,827 (19.57) |
11,475 (20.15) |
|
|
29 - 30 |
5,287 (27.03) |
13,077 (22.97) |
|
|
31 - 32 |
3,844 (19.66) |
8,387 (14.73) |
|
|
33 - 34 |
1,592 (8.14) |
3,383 (5.94) |
|
|
Birth Weight (grams) |
|
|
|
|
< 500 |
2,295 (7.44) |
11,530 (11.87) |
< 0.001 |
|
500 - 749 |
4,316 (13.99) |
18,063 (18.59) |
|
|
750 - 999 |
4,703 (15.24) |
17,299 (17.81) |
|
|
1000 - 1249 |
7,425 (24.06) |
21,195 (21.82) |
|
|
1250 - 1499 |
11,354 (36.80) |
26,857 (27.65) |
|
|
Intraventricular Hemorrhage |
3,771 (12.22) |
12,465 (12.83) |
0.005 |
|
Severe IVH |
854 (33.10) |
2,539 (30.93) |
< 0.001 |
|
Respiratory Distress |
17,779 (57.62) |
51,370 (52.88) |
< 0.001 |
|
Cesarean Section |
23,380 (75.77) |
53,824 (55.40) |
< 0.001 |
|
Severe Asphyxia |
174 (0.56) |
790 (0.81) |
< 0.001 |
|
Pulmonary Hemorrhage |
659 (2.14) |
1,636 (1.68) |
< 0.001 |
|
Patent Ductus Arteriosus |
6,089 (19.73) |
15,171 (15.62) |
< 0.001 |
|
Apnea of Prematurity |
7,474 (24.22) |
18,376 (18.92) |
< 0.001 |
|
Pneumothorax |
1,616 (5.24) |
4,463 (4.59) |
< 0.001 |
|
Anemia of Prematurity |
11,171 (36.20) |
30,601 (31.50) |
< 0.001 |
|
Maternal Hypertension |
359 (1.16) |
2,484 (2.56) |
< 0.001 |
|
Breech presentation |
252 (0.82) |
600 (0.62) |
< 0.001 |
|
Renal Failure |
462 (1.50) |
1,370 (1.41) |
< 0.001 |
Table 1: Demographic and clinical characteristics of the very low birth weight infants population stratified by maternal gestation type.
Overall, black infants were 12% more likely than white infants to have IVH (p < 0.001). Females had a 19% lower risk of IVH than males (p < 0.001). Unadjusted risks increased as gestational age decreased. Cesarean deliveries presented as a protective effect, as they were 15% less likely than non-C-section deliveries to result in IVH. This ratio was observed within the twin and singleton subgroups as well. Babies with respiratory distress syndrome were 3 times as likely of developing IVH than those without respiratory distress syndrome (p < 0.001). Severe asphyxia increased the risk of IVH by 53% (p < .0001). Pulmonary hemorrhage also showed a strong association to IVH. Infants with pulmonary hemorrhage were 4.7 times as likely to develop IVH versus infants without (p < 0.001). Infants with anemia was 70% more likely to have in IVH (p < 0.001). A pneumothorax diagnosis was 3 times more likely to result in IVH (p < 0.001) versus not having pneumothorax and having renal failure also presented significantly increased risks of IVH. Mothers with hypertension were 45% less likely to have a child with IVH (p < 0.001).
Before controlling for the other predictors, twins had a 14% decreased risk of IVH than singleton infants (p < 0.001). After adjusting for predictors (Table 2), twins still had a decreased risk (12%) of IVH (p < 0.001). In the adjusted model, male infants had a greater risk of developing IVH than females (p < 0.001). C-sections were 29% less likely to result in IVH (p < 0.001). Infants with RDS were twice as likely of developing IVH as those without (p < 0.001). Infants with pulmonary hemorrhage were 3 times as likely to develop IVH compared to infants without (p < 0.001). Anemia had a 39% increased risk (p < 0.001) of developing IVH. Maternal hypertension presented decreased risks for IVH. Among infants with IVH, twins had an increased risk of severe IVH (Figure 2).
|
|
Unadjusted OR (95% CI) |
p value |
Adjusted OR (95% CI) |
p value |
|
Twin |
0.86 (0.79 - 0.93) |
< 0.001 |
0.88 (0.82 - 0.94) |
< 0.001 |
|
Female |
0.80 (0.75 - 0.86) |
< 0.001 |
0.85 (0.80 - 0.90) |
< 0.001 |
|
Cesarean Section |
0.8498 (0.79 - 0.92) |
< 0.001 |
0.71 (0.66 - 0.76) |
< 0.001 |
|
Respiratory Distress Syndrome |
3.04 (2.74 - 3.37) |
< 0.001 |
2.38 (2.16 - 2.63) |
< 0.001 |
|
Severe Asphyxia |
1.53 (1.14 - 2.06) |
< 0.001 |
1.25 (0.97 - 1.62) |
0.09 |
|
Pulmonary Hemorrhage |
4.70 (3.99 - 5.52) |
< 0.001 |
3.06 (2.64 - 3.56) |
< 0.001 |
|
Apnea |
0.97 (0.88 - 1.07) |
0.51 |
0.89 (0.82 - 0.97) |
0.006 |
|
Pneumothorax |
3.07 (2.75 - 3.43) |
< 0.001 |
1.48 (1.2 - 1.80) |
< 0.001 |
|
Anemia |
1.69 (1.54 - 1.86) |
< 0.001 |
1.39 (1.28 - 1.52) |
< 0.001 |
|
Maternal Hypertension |
0.55 (0.37 - 0.81) |
0.003 |
0.68 (0.50 - 0.93) |
0.02 |
|
Breech presentation |
0.54 (0.31 - 0.95) |
0.03 |
0.61 (0.39 - 0.95) |
0.03 |
|
Renal Failure |
3.34 (2.74 - 4.06) |
< 0.001 |
2.08 (1.72 - 2.50) |
< 0.001 |
Table 2: Unadjusted and adjusted multivariable models: Odds ratio of having IVH for demographic and clinical predictors of the entire VLBW preterm infant population.
Figure 2: Adjusted odds ratios of intraventricular hemorrhage and severe intraventricular hemorrhage in Twins vs. Singletons.
Our findings show that twin gestations have a lower risk of IVH than singleton births and that many factors should be considered when analyzing IVH risk. The predictors that were included in the multivariate model are conditions that are present at delivery and before IVH occurrence. Male gender, vaginal delivery, respiratory distress syndrome, pulmonary hemorrhage, pneumothorax, anemia and renal failure are suggested as risk factors for IVH. Efforts to prevent IVH have focused on preventing prematurity as that is the greatest cause of IVH. These findings show that managing these other conditions soon after delivery may also reduce the risk of IVH.
The association between twin gestation and decreased IVH risk and the overall decrease in IVH incidence and mortality are potentially due to neonatal and obstetric care advances over the last few decades. The transfer of high-risk mothers to tertiary care centers has improved outcomes [11-13]. Tocolytic therapy has been shown to delay preterm delivery long enough in order for the mother to receive specialized care [14]. Babies born in facilities with neonatal intensive care units (NICUs) have a lower risk of IVH than those who have to be transferred postnatally [15]. Perinatal use of corticosteroids and magnesium sulfate have been proven to reduce IVH risk when taken by mothers expecting to give birth preterm [16,17]. Corticosteroids improve survival of preterm infants by accelerating fetal lung development. Magnesium sulfate is used to slow uterine contractions and treat preeclampsia [16]. Delayed cord clamping has shown a protective effect against IVH [18]. Also, optimal resuscitation techniques and the use of indomethacin to treat patent ductus arteriosus have proven to reduce the risk of IVH [19]. Caesarean section delivery was a protective factor for IVH and other studies have also identified C-sections as having decreased risk [20-24]. This could have also contributed to the lower risk among twins because twins are more likely to be delivered via C-section [20,21].
The sample size is large and the data is weighted which appropriately represents the preterm infant population. A stratified random sample of hospitals was drawn and then all discharges are included from each selected hospital. Taking into account the cluster of hospitals conveys the differences that may exist within and between the different hospitals in the dataset.
Its large sample size enables analyses of rare conditions [9]. The study may have been vulnerable to selection or sample bias due to the sampling method of the HCUP database. Only data for states participating in HCUP are included in the database. Also, being that this is an administrative dataset, it is prone to missing variables, coding errors, and misclassification due to human error. Cranial ultrasounds are used to diagnose infants with IVH. Typically, these are performed a few days after birth so IVH cases of infants who died soon after birth may not be represented. This data does not identify when the diagnostic tests were performed for each subject. Furthermore, various studies have reported increased and comparable adverse neonatal outcomes in assisted reproductive technology conceived versus spontaneous conception pregnancies [23-29]. This data does not specify the type of conception for each subject. As previously noted, maternal perinatal administration of corticosteroids and magnesium sulfate have been shown to reduce the risk IVH in preterm infants [16]. Mothers’ of subjects who received corticosteroids and/or magnesium sulfate were not identified in this data.
The analyses resulted in many significant associations between conditions present at birth and IVH occurrence. Also, IVH is categorized into four different grades based on the degree of bleeding. Results suggest that among infants with IVH, twins have a higher prevalence of being diagnosed with grades III and IV (severe IVH). Further studies are necessary to determine whether gestation type can be used to predict IVH severity. Although twins were at a decreased risk of IVH in this study, it would still be interesting to research whether higher order (triplet or more) multiple gestations present a difference in IVH risk.
Authors declare no financial conflicts in relation to this manuscript.
Authors declare no conflict of interest in relation to this manuscript.
Copyright: © 2021 Mohamed A Mohamed., et al This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff








